Introduction
Dentigerous cysts, also known as follicular cyst is an developmental odontogenic cyst associated with impacted tooth with frequency estimation of 1.44 in every 100 unerupted teeth.1, 2 Dentigerous cysts are the second most common among developmental odontogenic cysts that develops as a result of fluid accumulation between the reduced enamel epithelium and crown of unerupted tooth at cemento-enamel junction. It commonly affects males as compared to the females with high frequency among 2nd to 4th decades.3, 4, 5 Dentigerous cysts commonly occur in permanent dentition and is uncommon in childhood. Among 75% cases located in the mandible, it commonly involves mandibular third molars, maxillary third molar, maxillary canine and mandibular second premolars.6, 7
The dentigerous cysts are usually asymptomatic unless it is inflamed/ infected and is mostly discovered on radiographs when tooth has failed to erupt or is missing.3, 8 Radiographic features of dentigerous cysts depicts unilocular radiolucent areas associated with crown of unerupted teeth with well-defined sclerotic margins unless infected.2, 9
Histopathologically, it is composed of thin fibrous cystic wall, with epithelial lining of non keratinized squamous epithelium resembling reduced enamel epithelium and is 2-4 layers thick.10 Treatment involves Enucleation alongwith removal of the associated tooth and the large cyst is treated by marsupialization. The prognosis of the dentigerous cyst is excellent and the lesion almost never recurs.11, 12
Case Report
A 40- year old female presented with swelling of right side of lower jaw present since one month. On examination, slight facial asymmetry was presented with respect to right lower jaw. Complete history was taken and it was reported by the patient that the swelling is painful since a week during mastication. Medical history was unremarkable.
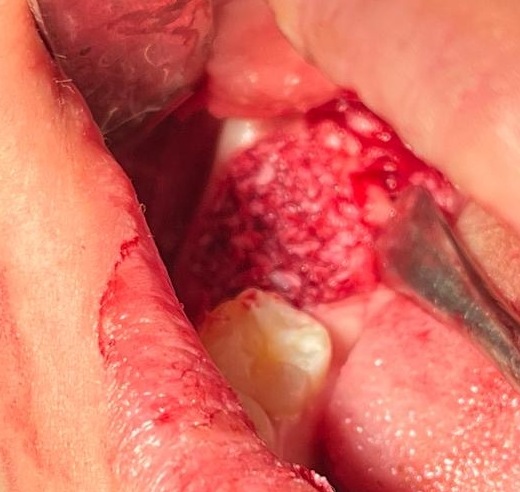
Intraoral examination revealed a swelling over right lower third molar area which on palpation was firm and there was no discharge of pus or any inflammatory signs from the site. Orthopantomogram revealed a radiolucency around right lower impacted third molar (Figure 1). The radiolucency was well-circumscribed and unilocular. Our clinical diagnosis was Dentigerous Cyst.

Under Local anesthesia, cystic enucleation (Figure 2) was performed for the removal of the cyst followed by bone grafting with bovine noble creos bone graft (Figure 4, Figure 5). Creos xenoprotect membrane was used for the protection of the nerve and guided tissue regeneration (Figure 3). The cystic lining was later sent for histopathological examination.


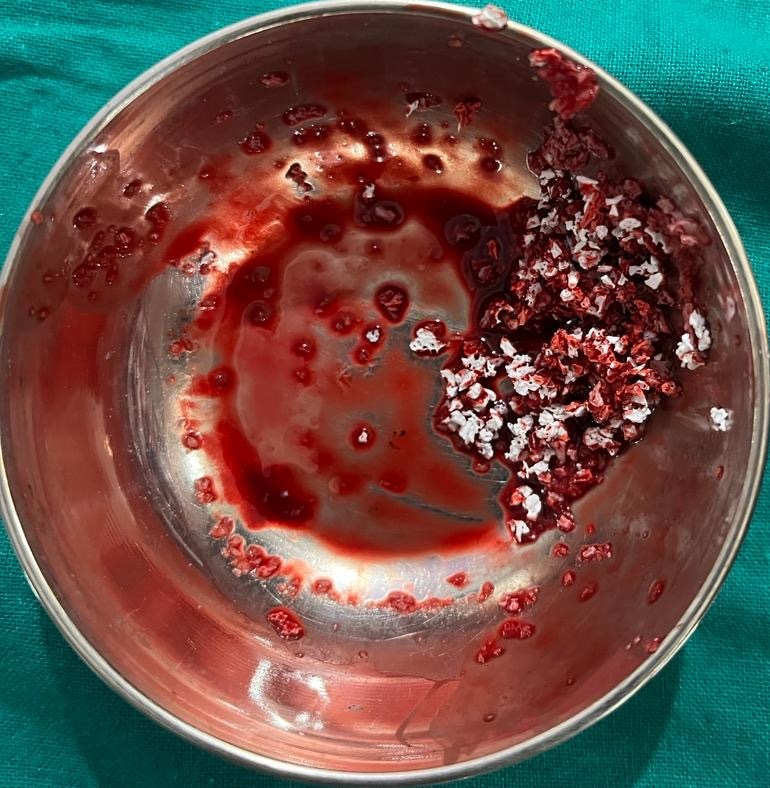
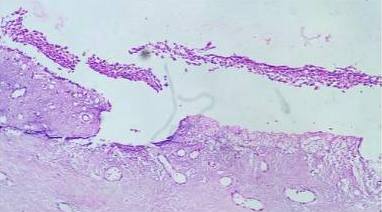
Macroscopically, Soft tissue specimen measuring approximately 1.5cm x 1cm and 5mm x 5mm, pale brown in color, soft in consistency was sent for the histopathological examination and microscopic examination revealed cystic lining of stratified squamous epithelium, 3-4 layer thick with the presence of bony trabeculae and dystrophic calcifications in addition with intense inflammatory cells. The above findings were suggestive of dentigerous cyst. There was no evidence of malignancy seen (Figure 6).
The post-operative examination revealed complete recovery without any complications and the patient was advised for the regular follow-ups. After 3 months, Implant placement followed by fabrication of crown was done to restore the function and orthopantomograph was performed after 6 months and the radiographic findings revealed successful bone regeneration and healing (Figure 7).

Discussion
Dentigerous cysts are the second most common odontogenic cysts, frequently found in mandible with more prevalence among males.2, 3, 7 It is associated mainly with crown of impacted tooth and may grow into a larger size before getting diagnosed. It is only painful when infected and mostly discovered during routine radiographs.1, 2, 5
The clinical presentation of dentigerous cyst depicts that the cyst is asymptomatic and remains undiagnosed by the patient until accidently diagnosed or becomes infected. It is a slow-growing, benign odontogenic cyst which may be developmental or inflammatory in origin. The exact etiology remains unclear but various theories were put forward to explain the pathogenesis of dentigerous cyst. Among those, one theory suggests that when the tooth is erupting, it exerts pressure on its follicle leading to fluid accumulation between reduced enamel epithelium and the crown of that tooth. Another theory suggests that it is caused due to inflammation at the apex of deciduous tooth which stimulates the developing permanent tooth germ and leads to accumulation of fluid.2, 7, 10, 13
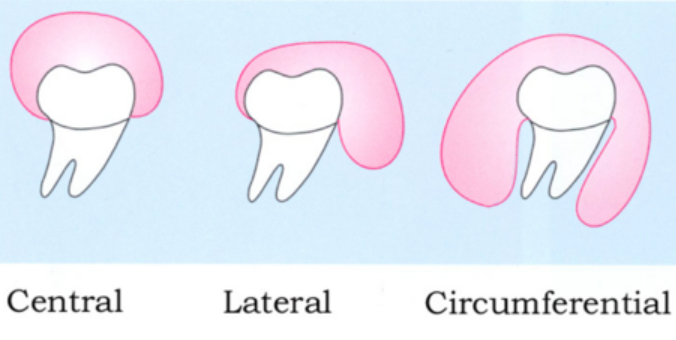
Radiographically, three radiological variations of Dentigerous cyst are observed (Figure 8).
Central variety: Most common and characterized by symmetrical radiolucent cavity enveloping the crown of unerupted tooth.
Lateral variety: Radiological appearance present laterally along the root surface as a result of follicle dilation on one aspect of the crown, partially covering crown of unerupted tooth.
Circumferential type: Cyst envelops the entire tooth due to follicle expansion occurring in this manner.1, 14
Cyst expansion takes place through the increase in hydrostatic pressure of its contents and it is unicentric expansion. The presence of inflammatory cells also play role in rise of intracystic osmotic tension leading to further expansion of the cyst.15, 16
Erupting tooth → Pressure on impacted follicle → Venous stasis → Transudation of serum → Increase in hydrostatic pressure → Cyst expansion.
Microscopic features of dentigerous cyst consists of cystic lining of stratified squamous epithelium. Rete peg formation is observed alongwith thickening of cystic epithelial lining in cases where the cyst is secondarily infected.16, 17 The underlying connective tissue may be fibrous or myxomatous and consists of thin epithelial lining which is 2-4 layers thick in case of dentigerous cyst whereas when the cyst became infected/inflamed, it exhibits inflammatory cells, mucus producing cells and occasional dystrophic calcifications might be observed.18
The Differential Diagnosis for dentigerous cyst involves Unicystic ameloblastoma, adenomatoid odontogenic tumor (AOT), Odontogenic Keratocyst (OKC).12, 17 The differentiation between unicystic ameloblastoma and dentigerous cyst depicts that unicystic ameloblastoma grows laterally whereas in dentigerous cyst, expansion of buccal cortex takes place as cyst grows buccally.19 To rule out adenomatoid odontogenic tumor, radiographic radiolucency plays a role. AOT is seen often in maxilla anterior and the radiolucency involves both coronal and radicular aspect of the involved tooth whereas in dentigerous cyst only coronal aspect of the impacted tooth is involved.20 Histological evaluation is the main criteria for ruling out Odontogenic Keratocyst from dentigerous cyst.21
Management of the dentigerous cyst involves proper assessment and is based on the age of the patient, size and location of the cyst and engaged vital structures.22 The treatment modalities of the dentigerous cyst includes enucleation of the cyst with or without removal of the involved tooth. When the cyst if of larger size, marsupialization is the treatment of choice. Another procedure is Decompression of the cyst in which the excision of the cyst is done once it shrinks in order to preserve the involved tooth.11, 12, 22