- Visibility 197 Views
- Downloads 40 Downloads
- Permissions
- DOI 10.18231/j.ijohd.2024.038
-
CrossMark

Perception and awareness of personal dental appearance and profile among dental students comparing index of orthodontic treatment needs with soft tissue silhouettes
- Author Details:
-
 Sharvari Anand Kangarkar *
Sharvari Anand Kangarkar *
-
Sheetal Suraj Yamyar
Abstract
Aim and Objectives: The purpose of this study was to compare the dental student’s and orthodontist’s perception on the aesthetic component of IOTN and soft tissue profile as well to assess which year student’s perception is closest to orthodontist. Also the association among dental health component (DHC) and aesthetic component(AC) component of IOTN was assessed by orthodontists.
Materials and Methods: The present study was conducted on 400 dental students (I, II, III, IV year ) of CSMSS dental college, aged 18-23 years. The Dental Health Component (DHC) and Aesthetic Component (AC) were recorded as defined by Brook and Shaw, with slight modification for AC assessment.The soft tissue profile perception was checked using 1 image from among 5 profile silhouettes. Clinical examination was carried out at CSMSS Dental College & Hospital, Aurangabad by the orthodontist.
Results: Unpaired T test showed statistically significant correlation among students and orthodontist perception regarding AC of IOTN and soft tissue profile. Pearson correlation coefficient statistically significant correlation among DHC and AC of IOTN among I, II and III year but not for final year. ANOVA test was used to find interclass correlation and showed that III and IV year student’s perception were closer to that of orthodontist’s perception.
Conclusion: The results of this study showed that dissatisfaction with personal dental appearance was not related to DHC. Also this study concluded that with progress of the curriculum from I to IV year the knowledge gained by students helped them to develop perception which was closer to that of orthodontists.
Introduction
The second most common dental abnormality is malocclusion. It could be detrimental to a person's psychosocial health, mandibular function, speech or dentofacial aesthetics, making it difficult for them to meet their functional needs and compromising their overall well-being.[1] Basic knowledge about treatment needs is necessary for orthodontic treatment to become a crucial component of oral health care programs. The requirement for treatment is determined by a variety of circumstances, including socioeconomic status, cultural background, health care system and the frequency of malocclusion. Decisions about the orthodontic services to be rendered, the need for training for human resources, the layout of treatment facilities, oral health professionals' continuing education, public health initiatives, screening for treatment priority and resource allocation can all be influenced by information on the perception of malocclusion. Additionally, this information can be used to enlighten and educate patients.[2] From a clinician's perspective, the necessity for orthodontic treatment has been measured using epidemiological indices. Planning for health services and population trend monitoring depend on these kinds of measurements.[3] A number of indices have been created in an effort to classify malocclusion into categories based on the severity of treatment requirements. The handicapping malocclusion assessment record,[4] the treatment priority index,[5] and the occlusal index[6] are a few examples of these. But in order to determine which people would benefit from orthodontic treatment, The Index of Orthodontic Treatment Needs ranks malocclusion according to the importance of different occlusal features for the person's dental health and perceived aesthetic impairment.[7] The Swedish Dental Health Board's index and the SCAN scale (Standardized Continum of Aesthetic Need; Evans and Shaw, 1987) were combined to create the IOTN (Linder-Aronson, 1974). The dental health component (DHC) and the aesthetic component (AC) make up the two components of the index.[2] Orthodontists and laypeople have different opinions about aesthetics. Guidelines, conventions and optimum ratios and angles help to make the professional opinions of orthodontists about dentofacial esthetics more objective. However, laypeople's impressions are primarily shaped by subjective emotions, such as the "beauty culture" prevalent in their peer groups and societal conventions generally. The self-perceptions of young adults are significant indicators when opting to undergo orthodontic treatment, as patients must derive satisfaction from enhancing their esthetics. This may supplement traditional clinical examination.[8] Numerous research were conducted in India to evaluate the reliability of IOTN, but none made a comparison between it and the soft tissue profile. Thus, the purpose of this study is to evaluate people's subjective perceptions of aesthetics and compare them to those of orthodontists.
Aims and Objectives
To compare orthodontist’s perception on aesthetic component of IOTN with dental student’s perception.
To find correlation between orthodontist’s perception of dental health component and aesthetic component of IOTN among I,II, III, IV year students.
To compare orthodontist’s perception of facial profiles and dental esthetics using soft tissue profile silhouettes with dental student’s perception.
Interclass comparison among I, II, III, IV year students regarding aesthetic component of IOTN and Soft tissue profile silhouettes and analyzing which class’s perception is closer to that of orthodontist’s perception.
Materials and Methods
The current study was carried out at the CSMSS Dental College in Aurangabad, Maharashtra, India at the Department of Orthodontics and Dentofacial orthopedics. The core of the sample consisted of 400 dental students, both male and female, in their first and final year and ages 18 to 23. The oral examination was conducted with prior approval from the institutional ethics committee. In order to prevent any ethical conflicts, the study's participants' identities were kept private. The study excluded patients who were receiving orthodontic treatment or who had finished it. For the sake of ease of statistical analysis, this study was divided into two groups: Group 1 was made up of dental students, while Group 2 was made up of orthodontists.
Comparison was done among perception for aesthetic component (AC) and soft tissue component between Group 1 and Group 2.
Correlation between orthodontist’s perception of dental health component and aesthetic component of IOTN among I,II, III, IV year students was established.
Comparison was done among orthodontist’s perception of facial profiles and dental esthetics using soft tissue profile silhouettes with dental student’s perception.
Interclass comparison among I,II, III, IV year students regarding aesthetic component of IOTN and Soft tissue profile silhouettes and analyzing which class’s perception is closer to that of orthodontist’s perception.
Assessment of AC
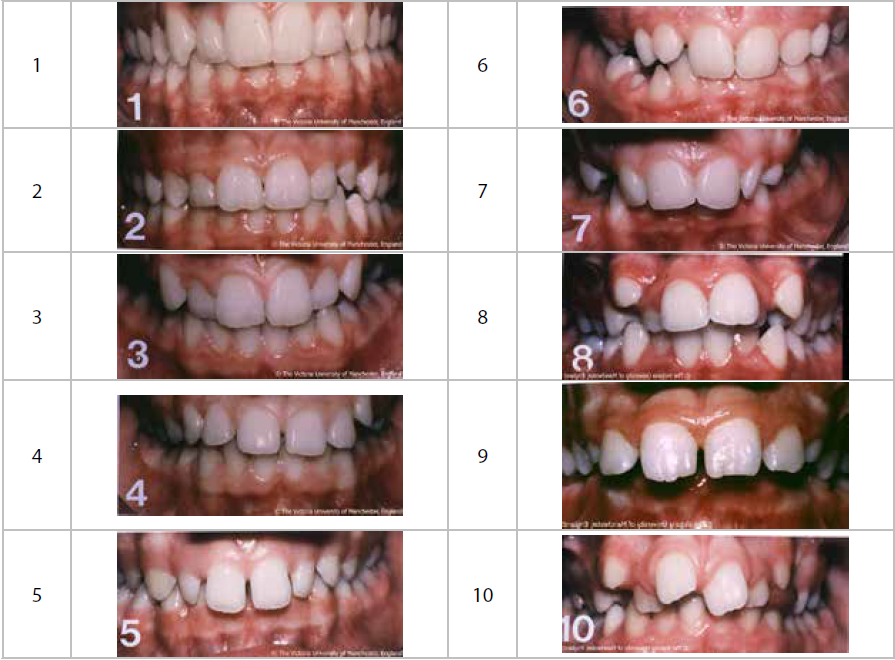
To evaluate the aesthetics component of the IOTN, ten color images ([Figure 1]) were displayed in a "power point presentation" to each dental student. Originally, Evans and Shaw used this series of images as part of their 1987 SCAN Index, or Standardized Continuum of Aesthetic Need.[9] Every student was instructed to assess their attractiveness by comparing their teeth to the standard photos and assigning a score to the photo that most closely resembled theirs. The student's score was used to determine the grade. The orthodontist's assessment of the students' looks was also documented. To make recording and tabulation easier, the scale was changed from the original ten-point SCAN Index rating system of "0.5 to 5" to ten-point SCAN Index scoring system of "Grade 1 (most appealing) to Grade 10 (least attractive). The following questions were asked (Lunn et. al 1993).This set of ten images illustrates a variety of dental attractiveness; the most appealing tooth arrangement is number 1 and the least attractive tooth arrangement is number 10. On this scale, where would you place your teeth? The orthodontist used disposable gloves for the examination, which was conducted in full daylight using a mouth mirror, fine explorer and a half-millimeter ruler. The purpose of the records was to record the Dental Health Component (DHC) and Aesthetic Component (AC) in order to determine the need for treatment based on IOTN. Orthodontists also analyzed the soft tissue profile.
Assessment of DHC
The following occlusal traits—MOCDO, or missing teeth, overjet, crossbite, displacement and overbite—were examined in order to document the dental health component. The following Performa, which was first used by Brook and Shaw, was used to define each of the five DHC grades. The "Dental Health Component," which was first utilized in the study to produce the Index of Orthodontic Treatment Need, was the basis for the grading.[7] The DHC grades were as follows:
Grade 1: No need for Orthodontic treatment.
Grade 2: Little need for Orthodontic treatment.
Grade 3: Moderate need for Orthodontic treatment.
Grade 4: Great need for Orthodontic treatment.
Grade 5: Very great need for Orthodontic treatment.[7]
The severe most malocclusion trait decided the grade for DHC of IOTN for an individual.
Assessment of soft tissue profile
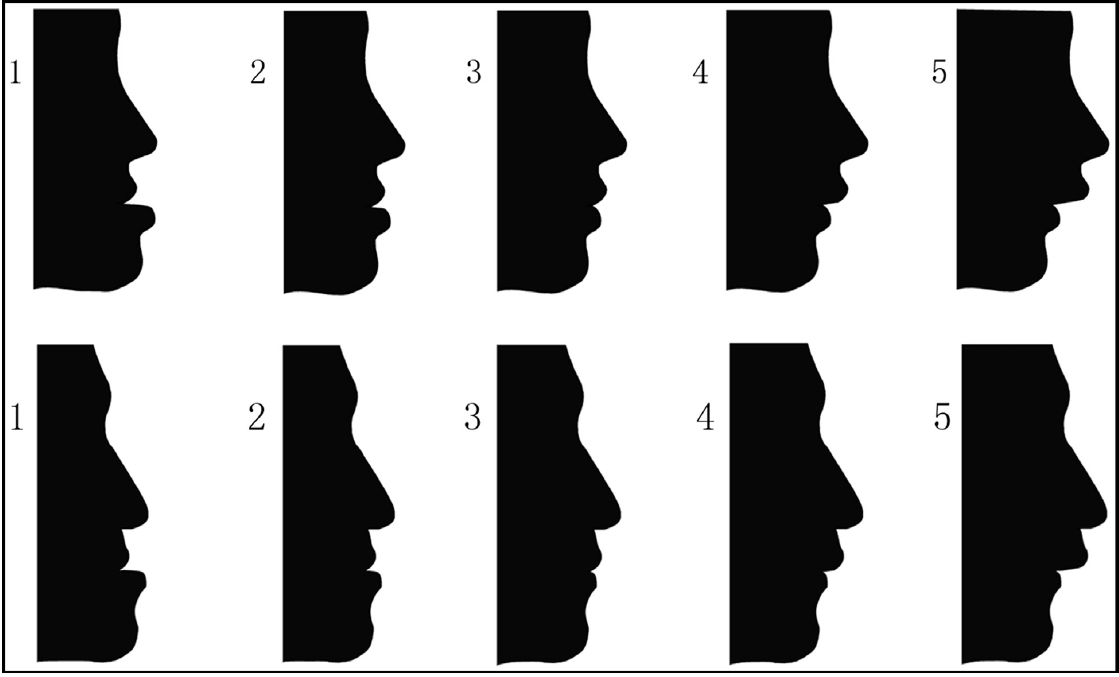
First, using Photoshop (CS 8.0.1; Adobe Systems, San Jose, Calif), sample straight-profile silhouettes of male and female individuals were produced, following landmarks that were chosen based on widely accepted standards of soft tissue measurements ([Figure 1]). In general, straight profiles are thought to be the best for facial aesthetics. An additional set of profile silhouettes was then created by modifying the original position of the pogonion, which was protruded and then retruded by 6 and 12° from the straight profiles, based on 2 straight profile silhouettes for males and females ([Figure 2]). To preserve sex distinctions and soft-tissue continuity, the alterations were artistically tweaked. Two sets of male and female profile photos were created from the altered silhouettes. The following were the profiles' scores: The first five are severe concave, followed by mild concave, straight, mild convex and severe convex.[10] Using a face mirror and an image of silhouettes, the dental students were asked to grade their soft tissue profiles on a scale of 1 to 5, which was then compared to the orthodontist's soft tissue profile score.
Results
Using an unpaired T test, the current study evaluated the opinions of orthodontists and dental students about the aesthetic component of IOTN ([Table 1]). The mean AC score for the orthodontist was 2.24±1.573, while the student's AC score was 1.98±1.295. A statistically significant P value of 0.002 was determined. Pearson's correlation coefficient was utilized to determine the relationship between orthodontists' assessments of the aesthetic and dental health components of IOTN among students in the first, second, third and fourth years of study. DHC and AC were observed to be statistically significantly correlated in the first year (p<0.001; r=.578), second year (p<0.001; r=.565) and third year (p=0.001; r=.589), but not in the fourth year (p=0.344; r=.179) ([Table 2]). Using soft tissue profile silhouettes, an unpaired t test was performed to evaluate orthodontists' perceptions of facial profiles and dental esthetics. The results demonstrated a substantial association between orthodontists' and students' perceptions of soft tissue profile, with a P value of 0.001 ([Table 3]). The AC component of IOTN was tested using the Anova test to determine the interclass correlation among I, II, III and IV year students. The results showed that there was no significant connection between the four classes' perceptions of the aesthetic component of IOTN, with a P value of 0.103 ([Table 4]). Similar to this, an Anova test was conducted to determine the interclass correlation for soft tissue perception utilizing profile silhouettes across students in years I, II, III and IV. A significant p value of 0.001 was discovered ([Table 5]). The correlation between all four classes and the orthodontists' perception of the AC component of IOTN was examined using an unpaired T test. The results indicated that the fourth year students had a closer perception of the AC component, while the third year students had a closer perception of the Profile component, as compared to orthodontist’s perception ([Table 6]).
|
|
AC orthodontist |
AC students |
Mean difference |
t test |
p value |
|
Mean Score |
2.24± 1.573 |
1.98± 1.295 |
0.265± 1.002 |
-3.209 |
0.002* |
|
|
Year |
Pearson’s correlation coefficient (r) |
P value |
|
DHC Vs AC |
1st year |
0.578 |
<0.001* |
|
|
2nd year |
0.565 |
<0.001* |
|
|
3rd year |
0.589 |
0.001* |
|
|
4th year |
0.179 |
0.344 |
There was statistically significant correlation was found between DHC and AC among 1st year with p<0.001; r=0.578
There was statistically significant correlation was found between DHC and AC among 2nd year with p<0.001; r=0.565
There was statistically significant correlation was found between DHC and AC among 3rd year with p=0.001; r=0.589
There was statistically insignificant correlation was found between DHC and AC among 4th year with p=0.344; r=0.179
|
|
Profile orthodontist |
DHC |
Mean difference |
t |
p value |
|
Mean Score |
2.97±.932 |
2.050± 1.0474 |
0.9156± 1.1823 |
9.390 |
<0.001* |
|
|
N |
Mean |
Std. deviation |
Std. error |
95% Confidence interval for mean |
F |
ANOVA p value |
|
|
Lower bound |
Upper bound |
|||||||
|
1st year |
50 |
2.12 |
1.507 |
0.213 |
1.69 |
2.55 |
2.098 |
0.103 |
|
2nd year |
37 |
1.89 |
1.370 |
0.225 |
1.44 |
2.35 |
||
|
3rd year |
30 |
1.53 |
0.937 |
0.171 |
1.18 |
1.88 |
||
|
4th year |
30 |
2.30 |
1.022 |
0.187 |
1.92 |
2.68 |
|
|
N |
Mean |
Std. deviation |
Std. error |
95% Confidence interval for mean |
F |
ANOVA p value |
|
|
Lower bound |
Upper bound |
|||||||
|
1st year |
50 |
2.90 |
.886 |
.125 |
2.65 |
3.15 |
9.361 |
<0.001* |
|
2nd year |
37 |
3.11 |
.516 |
.085 |
2.94 |
3.28 |
||
|
3rd year |
30 |
3.00 |
.263 |
.048 |
2.90 |
3.10 |
||
|
4th year |
30 |
2.20 |
1.031 |
.188 |
1.82 |
2.58 |
|
AC |
Orthodontic perception |
Mean difference |
p value |
|||
|
Class |
Mean |
SD |
Mean |
SD |
||
|
1st Year |
2.12 |
1.507 |
2.42 |
1.896 |
-0.300 |
0.092 |
|
2nd Year |
1.89 |
1.370 |
2.14 |
1.858 |
-0.243 |
0.203 |
|
3rd Year |
1.53 |
.937 |
1.83 |
0.973 |
-0.333 |
0.010* |
|
4th Year |
2.30 |
1.022 |
2.47 |
0.937 |
-0.167 |
0.167 |
|
Profile |
Orthodontic perception |
Mean difference |
p value |
|||
|
Class |
Mean |
SD |
Mean |
SD |
||
|
1st Year |
2.90 |
0.886 |
3.26 |
0.965 |
-0.360 |
0.069 |
|
2nd Year |
3.11 |
0.516 |
3.14 |
0.751 |
-0.027 |
0.860 |
|
3rd Year |
3.00 |
0.263 |
3.00 |
0.455 |
000 |
1.00 |
|
4th Year |
2.20 |
1.031 |
2.23 |
1.073 |
-0.033 |
0.823 |
Discussion
The motivation for most orthodontic procedures is the desire for treatment from people who are self-conscious about their appearance. Because of this, the orthodontist's goal is to guarantee the patient is satisfied with the results of therapy in addition to enhancing function and attractiveness. The success of orthodontic treatment depends on striking a balance between the patient's perceived demands and the orthodontist's objective assessment of the patient's orthodontic difficulties, since the orthodontist values the patient's satisfaction.[2] The evaluation of treatment needs is crucial for the following reasons: it gives information on workload, promotes logical decision-making regarding workforce requirements, aids in treatment facility design and helps public health dentists and related staff receive additional training.[10] However, earlier research employing the IOTN has shown that it can be challenging, especially for younger individuals, to allocate the aesthetic component scale to the "own" dentition.[11] For these reasons, a group of young students is selected for the current study. The photos of the aesthetic component show some of the distinctive characteristics of the occlusion at this point in dental development. The kids that underwent examination discovered these characteristics in their own teeth. This fact was thought to be beneficial for reliably evaluating aesthetics.[12] According to psychological reports, face attractiveness—especially in the oral region—is the most significant aspect of total appearance.[13] The majority of the children that were evaluated said they were happy with the way their teeth looked. Graber and Lucker (1980) achieved comparable outcomes.[14] Due to differences in their understanding of orthodontic treatment, younger and older students have varied perceptions of their personal dental appearance. Therefore, before developing an orthodontic care system, it is vital to evaluate the perceptual awareness of malocclusion.[2] The perception of AC of IOTN between orthodontists and dentistry students was shown to be statistically significant in the current study, with a P value of 0.002. According to several studies (Shaw et al., 1975, Prahl-anderson et al., 1979, Lindsay and Hodgins et al., 1983, Stenvik et al., 1997, Mandall et al., 2001, Hamdan et al., 2004), orthodontists view AC more critically than do laypeople or children.[15] This demonstrates that dental students know more about orthodontic treatment than other laypeople do, which leads to a perception more in line with an orthodontist's, which is consistent with the findings of a study by Siddiqui TA et al (2014).[16] A substantial correlation was established between the DHC and AC of students in their I, II and III years, but not among those in their IV year, based on a study of the correlation between DHC and AC for all students from I to IV year. The study's findings demonstrated that the degree of occlusal abnormalities was not in a linear relationship with dental appearance dissatisfaction. This result emphasizes that DHC could not be a significant factor to consider when assessing treatment requirement.[17] The canonic perspective of the face is typically derived from the frontal view rather than from less relevant perspectives like profile or bird's-eye views, according to Gestalt psychology theory. Orthodontists prefer to evaluate face profiles using cephalometric measurements since their professional training has shaped their views of profile esthetics. Their treatment programs and results are frequently designed to satisfy the more objective orthodontic norms and parameters, which alone represent the opinions of experts. Nonetheless, the cognitive dissonance theory contends that the way the general public views facial features is influenced by the "beauty culture" and social standards of their peer groups and the larger society. Furthermore, due to the influence of mass media, culture, geography, race, time, societal standards and "beauty culture" evolve. Consequently, the most significant influences on how a young adult perceives their face profile are not orthodontic norms but rather the norms of their peer groups and society.[8] The results of this investigation demonstrated a statistically significant association between the orthodontist's and dental students' perceptions of the same profile. Although the majority of students thought that image 3 was the most aesthetically pleasing, they also thought that images 2 and 4 were acceptable. The perception of esthetic profile differed between males and females, although this was not measured. ANOVA was used to compare classes and assess perceptions of soft tissue profiles and AC of IOTN among all four-year students. The results showed a statistically significant association between all four groups. These were then contrasted with the opinions of orthodontists, demonstrating that third year students had a closer perception of orthodontists about profile and fourth year students had a closer perception of orthodontists regarding AC.
Conclusion
The perceptions of I and II year students differed from III and IV year students and were closer to that of lay person. This concluded that as the students progressed from first to final year and with the increasing knowledge gained by them throughout the curriculum, their sense of aesthetic perception developed through dental point of view which was more in resemblance with orthodontist.
Ethical Approval
This study was conducted with prior approval from the CSMSS Dental College in Aurangabad, Maharashtra ethics committee.
Source of Funding
None.
Conflict of interest
None.
References
- Kharbanda O. What is the prevalence of malocclusion in India? Do we know Orthodontic treatment needs of our country. J Indian Orthod Soc. 1999;32(2):33-41. [Google Scholar]
- Hlaing E, Myo Y, Yee H, Win S. A study of Index of Orthodontic Treatment Need (IOTN) and perception of personal dental appearance among dental students. Myanmar Dent J. 2014;21(1):60-6. [Google Scholar]
- Ngom P, Diagne F, Dieye F, Diop-Ba K, Thiam F. Orthodontic treatment need and demand in Senegalese school children aged 12-13 years. An appraisal using IOTN and ICO. Angle Orthod. 2007;77(2):323-30. [Google Scholar]
- Griffiths G, Addy M. Effects of malalignment of teeth in the anterior segments on plaque accumulation. J Clin Periodontol . 1981;8(6):481-90. [Google Scholar]
- Ainamo J. Relationship between malalignment of the teeth and periodontal disease. Scand J Dent Res. 1972;80(2):104-10. [Google Scholar]
- Shaw W, Addy M, Ray C. Dental and social effects of malocclusion and effectivenessof orthodontic treatment: a review. Community Dent Oral Epidemiol. 1980;8(1):36-45. [Google Scholar]
- Shaw W, Richmond S, O'Brien K, Brook P, Stephens C. Quality control in orthodontics: Indices of treatment need and treatment standards. Br Dent J. 1991;170(3):107-12. [Google Scholar]
- Yin L, Jiangm, Chenw, Smales R, Tang WQ, L. Differences in facial profile and dental esthetic perceptions between young adults and orthodontists. American Journal of Orthodontics and Dentofacial Orthopedics. 2014;145(6):750-756. [Google Scholar]
- Evans R, Shaw W. Preliminary evaluation of an illustrated scale for rating dental attractiveness. Eur J Orthod. 1987;9(4):314-8. [Google Scholar]
- Bowden D, Davies A. Inter-and intra-examiner variability in assessment of Orthodontic treatment need. Community Dent Oral Epidemiol. 1975;3(4):198-200. [Google Scholar]
- Holmes A. The prevalence of orthodontic treatment need. Br J Orthod. 1992;19(3):177-82. [Google Scholar]
- Trivedi K, Shyagali T, Doshi J, Rajpara Y. Reliability of Aesthetic component of IOTN in the assessment of subjective orthodontic treatment need. J Adv Dent Res. 2011;2(1):59-65. [Google Scholar]
- Baldwin D. Appearance and aesthetics in oral health. Community Dent Oral Epidemiol. 1980;8(5):244-56. [Google Scholar]
- Graber L, Lucker G. Dental esthetic self-evaluation and satisfaction. Am J Orthod. 1980;77(2):163-73. [Google Scholar]
- Hamdan A. The relationship between patient, parent and clinician perceived need and normative Orthodontic treatment need. Eur J Orthod. 2004;26(3):265-71. [Google Scholar]
- Siddiqui T, Shaikh A, Fida M. Agreement between orthodontist and patient perception using Index of Orthodontic Treatment Need. Saudi Dent J. 2014;26(4):156-65. [Google Scholar]
- Yeh M, Koochek A, Vlaskalic V, Boyd R, Richmond S. The relationship of 2 professional occlusal indexes with patients' perceptions of aesthetics, function, speech, and orthodontic treatment need. Am J Orthod Dentofacial Orthop. 2000;118(4):421-8. [Google Scholar]