Introduction
Orthodontics as a specialty has its long run of existence and every time it comes through various profound and revolutionary changes in terms of diagnosis, treatment planning, biological and biomechanical applications. In contemporary orthodontics, retraction of teeth after extraction of premolars is an essential part of orthodontic treatment.1 Single-step-enmass retraction of 6 anterior teeth at once or two-step procedure in which canine has to retract first followed by retraction of 4 incisors are the most common routines to close the space created by the extraction of premolars.2 There is a number of methods those can be employed for the above said purpose. In modern orthodontics, solutions are available in the form of friction and frictionless mechanics.3 The frictional method includes the use of elastomeric materials, active tie-backs, coil springs (NiTi/ SS-stainless steel/ Elgiloy-Co-Cr-Ni) while frictionless method utilizes different configuration of loops or retraction spring made up of materials like TMA (β-titanium), SS, or elgiloy.4, 5, 6 Retraction via these methods required 4 to 5 months for full retraction of canine and almost always consume anchorage when used with conventional anchorage units like posterior teeth or enhancement of anchorage with palatal or lingual arches, that is why now a day TADs (Temporary Anchorage Devices/Miniscrews) are popular choice to facilitate retraction in terms of reducing anchorage loss.7 Total orthodontic treatment time is usually an average of about 20-24 months or even more and this is the most common reason that patient may lose confidence, motivation, and compliance towards the treatment procedures. Due to longer treatment time, researchers are now focusing to accelerate the tooth movement via the application of different invasive (Corticotomy, PAOO- Periodontally Accelerated Osteogenic Orthodontics, Peizocision, Dental/Dentoalveolar distraction), minimal invasive micro-osteo-perforations (MOPs) or non-invasive procedures (low level laser, vibrations, pulsed electromagnetic field, drugs and supplements).8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20 This article aims to provide the literature review of various methods of canine retraction followed by a report of 10 cases, focusing on canine retraction via various method available.
Review of Literature
Ray D Robinson was the first to introduce loop for retraction purposes long back during Angle era.21 Open and closed vertical loop came in existence around the year 1933 and later on became an integral part of edgewise mechanics.22 Segmental arch technique under frictionless mechanics was popularized by Burstone et al.6 The material of choice was TMA for construction of T loop, which is based on the application of differential moments between teeth. Differential moments are required to achieve particular tooth movement. These differential moments are classified as alpha (anterior) and beta (posterior) moments. Differential moments are used for obtaining differential anchorage, force system, and root movement.6 The PG retraction spring is another popular spring based on segmental arch mechanics, can be made from 0.016” x 0.022” stainless steel wire or TMA.23 Opus 70 loop is a closing loop design based on Castigliano's theorem for the derivation of moment to force ratio, best suited in continuous SS or TMA archwire. The opus loop works better than the other loops in most instances for both the centered and off-centered placements.24 A mushroom loop was fabricated by Nanda and It is similar to the design of T loop except that its apical area is curved.25 Location, moment generated, and spring characteristics of a closing loop are the three basic properties, which decide the performance of the loop.26 Effect of gable bends on loop was study by a researcher and it was concluded that first and second order gable bends in stainless steel triangular loops have uncoupled effects on the clinically critical M/F.27 It is a proven fact that T loop design results in force system closer to those required for translation while vertical loops produce higher forces but much lower M/F ratio at maximum activation that is not useful to carry out the translation.28
Bennett and Mclaughlin popularized the use of Active tie back (elastomeric module with ligature) for retraction during the development of their well known MBT philosophy.4 Activation of elastic module twice to their size can produce a force of up to 100 gram. Tie back has to be replaced every 5 to 6 weeks until full retraction of canine achieved.5 Elastomeric Chains are a convenient choice for sliding mechanics and commercially available in configurations of closed, short and long filament chains. E chains are easy to apply, relatively inexpensive, and no patient cooperation needed for insertion but rapid force degradation, relaxation, staining, and deformation are the major drawbacks.29 E chains has to be replaced in every 4 weeks or less.30 Closed coil springs produce more predictable and constant force than elastics. SS coils have high load deflection rate as compared to Ni-Ti coil springs. Ni-Ti close coil springs are efficient on constant production of force and useful to produce more consistent space closure than elastics. Coil springs are available in different sizes (eg. 6, 9, and 12mm) and their extension depends upon manufacturer’s recommendation.5 Just like elastics, these springs are also quick and easy to apply without patient co-operation. Major issues with sliding mechanics are the occurrence of friction and binding due to improper angulation of canine bracket to wire that leads to the production of unwanted forces.31 Rare earth magnets (e.g.- Parylene coated neodymium-iron boron=Nd2Fe14P) are less popular method for retraction of canine.32
An invasive procedure known as Dental Distraction was first performed by Liou, and Huang 13 for the purpose of rapid canine retraction. A different technique called Dento-Alveolar Distraction (DAD) for acceleration of canine distalization by performing osteotomies around the canines and achieved rapid tooth movement.14 This surgical technique did not rely on the stretching and widening of PDL thus prevents overloading and stress accumulation in the periodontal tissues. As DO is an extensive surgical procedure, further efforts have been made to refine the procedure which is less invasive to the patient. A new micro-invasive technique called micro-osteo-perforation has been introduced which literally translates to puncturing bone and stimulates cytokines activity which has been well scientifically proven. When an orthodontist creates micro-osteo-perforations in the alveolar bone, cytokines cascade is activated, resulting in a marked increase in osteoclast activity and bone remodeling. MOP can be completed inminutes and does not require advanced training. It causes less discomfort to the patients when compared to other surgical methods of accelerating tooth movement.15, 33 Periodontally Accelerated Osteogenic Orthodontics (PAOO) is a method to stimulate RAP (Regional Acceleratory Phenomenon) via conventional corticotomy and use of bone graft material.11 An alternative limited invasive procedure is known as Piezocision technique described in 2009 by Dibart et al.12 It combines cuts in the bone through the gingiva with a piezoelectric knife to create of submucosal tunnels for bone substitute material. According to the author, it is necessary to go through the entire cortical layer and reach the cancellous bone to stimulate RAP.12
Figure 1
Canine retraction via different methods: Case 1- NiTi coil spring; Case 2- SS coil spring; Case 3- canine retraction via PG spring; Case 4- canine retraction via T loop; Case 5- canine retraction via NiTi coil spring attached to sliding hook and anchorage enhancement from TADs; Case 6- canine retraction via E chain utilizing absolute anchorage from TADs; Case 7- canine retraction via active tie back; Case 8- canine retraction via E chain; Case 9- canine retraction via DAD procedure; Case 10- canine retraction via NiTi coil facilitated with MOPs

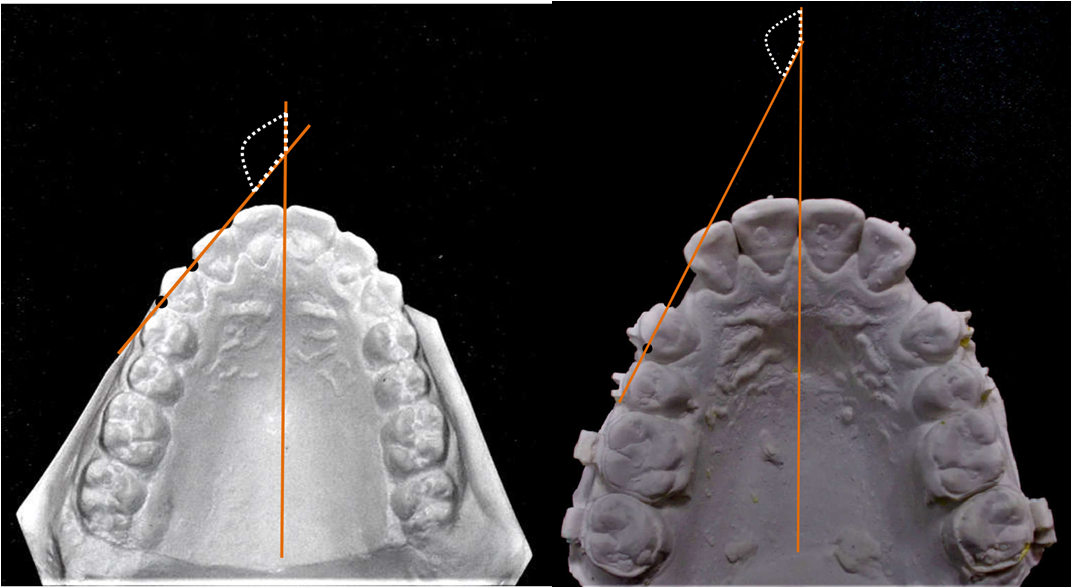
Figure 3
Pre and post retraction lateral cephalogram, and OPG radiographs (also used for measurement of distal tipping of retracted canines)
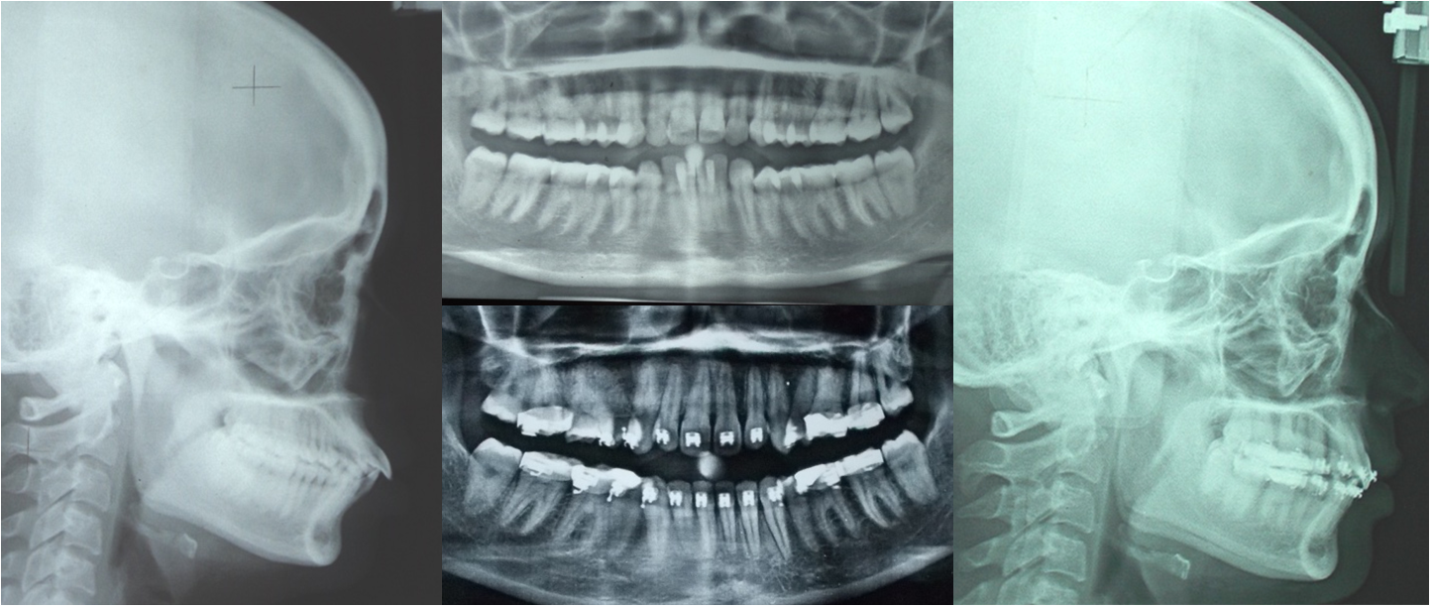
Figure 4
Amount of molar anchorage loss measured from superimposition of pre and post retraction lateral cephalogram tracings
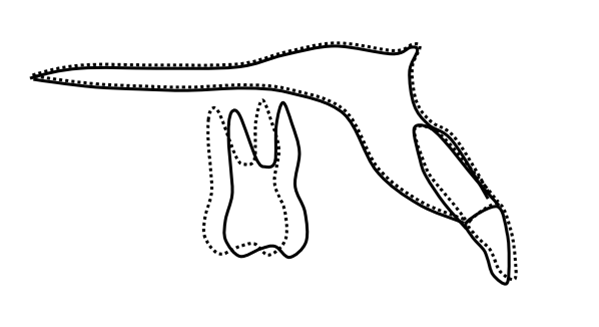
Table 1
Report of 10 cases of canine retraction via various methods
Table 2
Result after comparison of various methods with respect to different factors
|
Factors |
Results |
|
Rate of canine retraction |
DAD>MOPs>STN>TADE>PG spring>Tloop>Niticoil>S Scoil>Echain>ATB |
|
Anchorage loss |
ATB>Echain>SScoil>niticoil> Tloop>PGspring>MOPs>DAD> TADE=STN |
Commercially available AcceleDent device (OrthoAccel Technologies, USA) may generate a vibration of 0.25 N and a frequency of 30 Hz. In a study with AcceleDent device, it was shown that rapid retraction of canines with skeletal anchorage increased by 48.1% compared to the control group (1.16 mm vs 0.79 mm/month).34 Using electric toothbrush massage as a source of stimuli for 15 min a day at a frequency of 125 Hz leads to the acceleration of distal movement of canine (37.7% greater than in the control group).35 Photo-biomodulation technique involves the exposure of tissues to the effects of a therapeutic wavelength (600–1200 nm).36 Therapy with light can be divided into 2 basic types: low-intensity lasers (LIL), producing coherent light, and light-emitting diodes (LED), which are sources of incoherent light.37
Case Series
This case series is the presentation of 10 cases (age ranges from 15y to 19y) of canine retraction in premolar extraction space performed by 10 different methods of retractions to the patients enrolled in the Department of Orthodontics-Faculty of Dental Sciences at Banaras Hindu University. Although all the 4 canines retracted simultaneously after premolar extraction but only right maxillary canine is chosen for the comparison purpose. Mean right maxillary premolar extraction space was 6.4 mm. Each subject had 0.022x0.028 inch Victory (3M-Unitek) orthodontic brackets bonded. Active canine retraction did not commence until a 0.019x0.025-inch stainless steel archwire was engaged. Canine retractions consider being completed when canine contacted with the 2nd premolar (timing for root uprighting movement not calculated). Follow-ups were done after 3 weeks for each case except DAD, which is followed every day. Rate of canine retraction, and molar anchorage loss was noted in relation to right maxillary cuspid. Rotation of canine measures from the pre and post retraction dental casts as the angle formed between a line through the distal and mesial contact points of the canine, and the midpalatal raphe. Angulations (distal tip) are measured in orthopantomogram as the intersection of the midline and a line extending from the apex to crown tip of canine and compare it with the initial value. Loss of anchorage was determined from the superimposition of initial and post retraction lateral cephalogram tracings.
Discussion
Presented case series provide the valuable data regarding the rate of canine retraction, distopalatal canine rotation with respect to mid-palatine raphe, distal tipping of canine (angulation) with respect to the midline, and loss of molar anchorage when various canine retraction method employed. The mean force applied was 150±30 gms that is in the range with the study of Quinn, and Yoshikawa:38 Rate of canine retraction or any other tooth/teeth depends upon several factors. For example, alveolar bone density, hyalinization adjacent to the root area subjected to excess mechanical forces, or optimal force application produce frontal resorptions, as well as the magnitude of force applied.39, 40 Different methodology of force application are there in the literature to maximize the speed of orthodontic treatment via biologically sound response. When we used constant force (9mm) NiTi coil spring with conventional anchorage (Nance button) for cuspid retraction, the canine contacted the second premolar in 128 days and produces 1.7 mm of molar anchorage loss, 4 degree distoplalatal rotation and distal tipping of canine that is consistent with other studies reported.7, 41 When NiTi coil spring was used with sliding hook and absolute anchorage (TADs), canine retraction completed in 102 days with no anchorage loss and less angulation and rotational changes of canine. Same result was observed when TAD is used with E chain except for larger rotational and angular changes. Results with TADs are consistent with the study reported by Thiruvenktachari B et al. 7 The T-loop with a symmetric shape could be used to achieve a moment differential. Position of T loop was determined according to recommendation of Kuhlberg and Burnstone. 42 PG retraction spring was better in providing rotational control than T loop but no significant difference was there in terms of rate of canine retraction, angular changes and anchorage loss. Canine retraction was completed in 12 days via DAD procedure leaving a 4.5 degree distal tipping, 3 degree rotation and around 1 mm molar anchorage loss that is consistent with the study reported by Kurt et al and other. 43, 14 Canine retraction was increased when facilitated with MOPs but not as much as reported by Alikhani et al. and Sivarajan et al. 15, 44 Contradictory to above no significant increase in rate of canine retraction was observed by Amira et al and Alkebsi et al. 33, 45 Rate of canine retraction with the help of E chain and Active tie back was slower than the other method utilized and costs higher molar anchorage along with more rotational and angular changes were observed. Anchorage loss has occurred during canine retraction via all the methods employed except those facilitated with TADs. Geron et al 46 suggested that the majority of molar anchorage loss does not occur during canine retraction (33%), rather during incisor retraction when the Nance appliance is removed (67%) with a mean of 3.9±2.3 mm by the end of orthodontic treatment in patients treated with extraction of upper first premolars.
Conclusion
Fastest canine retraction was achieved by maximal invasive DAD procedure. MOPs ranks first in terms of rate of canine retraction in which minimal invasion is involved. Canine retractions, in which anchorage was taken from TADs rank best in terms of anchorage control. Minimal canine rotation was occurred in canine retraction with the help of PG spring. Minimal tipping was observed when canine retraction facilitates with MOPs. E chain and active tie back ranks worst in terms of all the said factors involved. The biggest limitation of the above presentation is that only one case was there under a particular method of canine retraction and so that results came after direct comparison should be taken carefully for any consideration.
Clinical Significance
Canine retractions facilitated with Micro-osteo perforation and temporary anchorage devices gave best result in terms of time taken for retraction and preservation of molar anchorage so use of these techniques would be beneficial during fixed orthodontic treatment. Use of active tie back and elastomeric chain should be better avoided during orthodontic treatment.