- Visibility 98 Views
- Downloads 10 Downloads
- DOI 10.18231/j.ijohd.2021.046
-
CrossMark

Furcal perforation repair using MTA — A clinical case series
Introduction
Perforation in the floor of the pulp chamber of multirooted teeth causes an inflammatory response in the periodontium, which can lead to irreversible loss of periodontal attachment in the area.[1] Pulp chamber perforations consist of internal or external root resorption, large carious lesion, and iatrogenic damages are some of the etiological factors involved.[2]
The alteration of furcation perforation can be attained by intracoronary or surgical approach. The root perforation can be treated surgically, a surgical attempt will often lead to pocket formation, loss of attachment, and periodontal furcation involvement.[3]
The prognosis may be questionable if radicular furcation is involved, but on the other hand the prognosis is usually good if diagnosed accurately and treated with a good material.[4] The prognosis is related more with the size, contamination location of the lesion.[5] The main principle of conservative furcal perforation treatment is to seal the defect with filling material as soon as possible.[6]
Mineral trioxide aggregate (MTA) was brought into market for the repairing lateral perforations by Loma Linda University in 1993.[7], [8] Various clinical applications such as management of Apexogenesis/apexification, internal root resorption, pulpotomy, repair of the root, pulp capping, and furcation perforations. MTA promotes dental tissue regeneration.[9] MTA is offering better microleakage safeguard than traditional endodontic repair.[10]
Researcher also established and observed some new cementum development adjacent to MTA which proves it to be superior than other endodontic materials. Thus making MTA is considered as a gold standard because of its unsurprising periodontal ligament (PDL) regeneration.[11] In this case series, 3 cases are described in which MTA was used to repair furcation perforation. Thus cases illustrate the potential benefits of MTA.
Case Series
Case 1
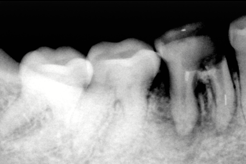
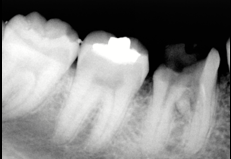
A 35-yr-old female patient reported to the dental clinican having chief complain of pain in her lower left back region since one month. On clinical examination a temporary dressing was observed with respect to 36, on percussion there was a pain. Restorative material was eliminated perforation was made and investigated clinically and radiographically. The mesial and the distal canals were cleaned and shaped in a crown down technique using ProTaper Rotary File Systems and with plentiful irrigation using 5.25% sodium hypochlorite and finally with 2% Chlorhexidine . Obturated with gutta-percha points and AH Plus using lateral condensation technique after selecting master cone. The perforation was sealed with mineral trioxide aggregate. In next appointment, MTA was applied and the tooth was temporary filled with Cavit temporary restoration material.
The patient was again resechulded after 24 hours to the department and it was found that there no signs or symptoms. Temporary sealing materials were removed and in this appointment, permanent restoration was done using Type GIC. In another appointment a full metal crown was given.
Radiographicall there is an evidence of bone formation adjacent to the MTA on three months with 6 months after treatment, radiography there was an osseous healing at the apex and the furcation



Case 2
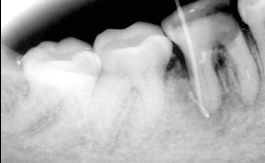
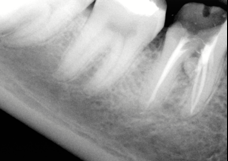
A fit and fine 27-Yr-old women came to the clinic with a history of incomplete root canal treatment 6 months back associated with pain in the lower back region.


On clinical examination it was observed there was no sensitivity on percussion and palpation Radiographically a little radiolucent area in furcal region with respect to 36 was observed. The caries and temporary restoration was eliminated.
Hemorrhage was restricted with plentiful irrigation with 1% sodium hypochlorite. The working lengths were determined with Raypex 5. The mesial and distal canals were cleaned and shaped in a crown-down technique using ProFile ISO files and plentiful irrigation with 5.25% sodium hypochlorite was done.
The root canals were obturated with gutta-percha points and AH 26 using the lateral condensation technique. MTA was then placed in the pulp chamber and the tooth was temporary Cavit temporary restoration material was filled. The patient recalled to the clinic three days later with no signs or symptoms . Now in another scheduled time, permanent restoration was done with the help of composite resin, in another appointment a full metal crown was given.
Case 3
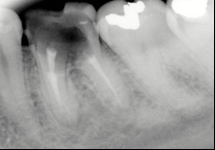
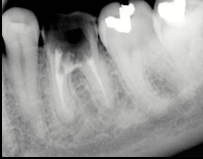
A 21-year female patient visited a dental clinic with grievance of pain on chewing and history of root canal treatment and crown 6 months before her visit.


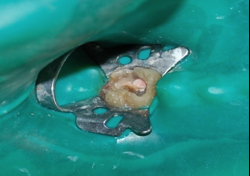
Several treatment options were disclosed to patient, among which patient opted for RCT along with repair of the perforation with MTA. The furcal perforation was definite by periapical radiography with respect to 46. RCT was completed, and irrigated with 1% sodium hypochloride. Grey MTA was applied. Radiographically when observed after ten days, the patient had no symptoms. After 6-month follow-up, a bone formation was evident.
Discussion
Furcal perforation is unwanted trouble which occur during RCT or post preparation. Equally, a danger of perforation may take place during elimination of affected tissue in a patient with caries that involves pulpal chamber. For ensuring a positive prognosis a siutation should be addressed quickly and immediately.[12] In the above 3 cases discussed , the problem was resolute without delay by application of MTA.
Main et al. used a material which has superb sealing properties (MTA) for 16 cases of perforation repair and found out that the material is very appropriate for repair of such perforations. Ferris and Baumgartner and in another study Hamad et al. also compared white and grey MTA and came to a conclusion that there was no disparity in their capability to seal perforations. On the other hand they established that significantly there was more leakage from an orthograde approach as compared with retrograde approach when perforations were repaired.[3]
Retention capacity of the MTA can be reduced so contamination should be avoided. Previous literature have declared that contact with adjoining tissues may boost the sealant capacity of MTA, as tissues have acidic environment which enhance this property. In the cases presented above, sealing of the lesions could be practical.[10] To put off overfilling or underfilling, one can use a resorbable collagen matrix before MTA application, depending upon on the size of the lesion. Although at hand, there is no size classification for furcal lesions to verify suitable treatment and prognosis so, all options are considered to have a fortified prognosis.[12]
Conclusion
Although use of MTA has been reported but literature on its success is restricted. Three familiar clinical presentations of perforation with relation to caries have been described above here. Even though the prognosis is better in case of smaller lesions MTA treatment is observed when radio graphically observed with good prognosis.
Source of Funding
None.
Conflict of Interest
None.
References
- M Samiee, M J Eghbal, M Parirokh, F M Abbas, S Asgary. Repair of furcal perforation using a new endodontic cement. Clin Oral Investig 2010. [Google Scholar]
- E B Bryan, G Woollard, W C Mitchell. Nonsurgical repair of furcal perforations: a literature review. Gen Dent 1999. [Google Scholar]
- S George, V Shivanna, N M Dhanyakumar. Calcium phosphate cement: A new saviour for furcation perforation? - An in-vitro study. Endodontology 2006. [Google Scholar]
- I Tsesis, Z Fuss. Diagnosis and treatment of accidental root perforations. Endod Top 2006. [Google Scholar] [Crossref]
- Z Fuss, M Trope. Root perforations: classification and treatment choices based on prognostic factors. Endod Dent Traumatol 1996. [Google Scholar] [Crossref]
- J C Ruddle, K M Hargreaves, L H Berman, . Nonsurgical endodontic retreatment. 2002. [Google Scholar]
- S J Lee, M Monsef, M Torabinejad. Sealing ability of a mineral trioxide aggregate for repair of lateral root perforations. J Endod 1993. [Google Scholar] [Crossref]
- G D Deus, C Reis, C Brandão, S Fidel, R A Fidel. The ability of Portland cement, MTA, and MTA Bio to prevent through-and-through fluid movement in repaired furcal perforations. J Endod 2007. [Google Scholar] [Crossref]
- M Torabinejad, N Chivian. Clinical application of mineral trioxide aggregate. J Endod 1999. [Google Scholar] [Crossref]
- M A Duarte, A C Demarchi, J C Yamashita, M C Kuga. Fraga Sde C. pH and calcium ion release of 2 root-end filling materials.. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003. [Google Scholar] [Crossref]
- A A R Hashem, E E Hassanien, M Proroot. MTA-Angelus and IRM Used to Repair Large Furcation Perforations: Sealability Study. J Endod 2008. [Google Scholar] [Crossref]
- Z Fuss, M Trope. Root perforations: classification and treatment choices based on prognostic factors. Endod Dent Traumatol 1996. [Google Scholar] [Crossref]