Introduction
The coronavirus disease 2019 (abbreviated “COVID-19”) is an emerging, rapidly spreading disease caused by a novel coronavirus and is known to give rise to illnesses ranging from the common cold to a severe acute respiratory syndrome (SARS).1 Initially termed as 2019-nCoV, the virus was later renamed as syndrome coronavirus 2 (SARS-CoV-2) by the International Committee on Taxonomy of Viruses (ICTV).2 The two unique features of this new virus that distinguishes it from other members of the coronavirus family such as SARS-CoV and MERS-CoV are low pathogenicity and high transmissibility.3 The most commonly observed clinical symptoms of the disease include fever, dry cough, fatigue, myalgia, and dyspnea. This new strain was first detected in December 2019 in Wuhan, Hubei Province, China. On 30 January 2020, the World Health Organization (WHO) declared COVID-19 as a public health emergency of international concern (PHEIC).4
CoV being a zoonotic pathogen can be transmitted via animal-to-human and human-to-human interactions.5 As viruses lack the properties of a living cell, they get activated and replicate only on entering the living cell of a host organism. Human-to-human transmission could be through droplet, feco-oral, or direct contact. In addition, it has been shown that corona virus survives on various inanimate surfaces for varying periods of time. This particular virus is known to have an incubation period of 2-14 days.6 The first week of March reported an alarmingly high number of new cases globally, and COVID-19 emerged as a pandemic and significant public health issue. As of 12 March 2020, there were more than 125,000 confirmed cases and around 4600 deaths across 118 countries around the world.6 The first case in India was however reported on January 30, 2020 in the state of Kerala. As of March 22, 2020, the number of cases in India rose above 300 and 7 deaths were reported according to the national health ministry. On March 24, 2020, the Government of India ordered a nationwide lockdown for 21 days initially, which was extended later limiting the movement of the entire 1.3 billion population there as a preventive measure against the COVID-19 pandemic. This included certain unprecedented measures such as the suspension of public transportation, the closing of public spaces, close management of communities, and isolation and care for infected people and suspected cases. All Indian residents, were also required to just stay at home to avoid contacting with others. The battle against COVID-19 is still continuing in India as its tally nears 53,000 and deaths have reached above 1,700.
No antiviral treatment or vaccine has been explicitly recommended for COVID-19 thus far. Therefore, taking all these factors into consideration, applying preventive measures to control COVID-19 infection is of utmost importance. Healthcare workers are inevitably the primary sector in contact with patients and among them, dentists are more prone to exposure due to infected cases in healthcare settings and are thus expected to be at high risk of infection.
By the end of January, the WHO and Centers for Disease Control and Prevention (CDC) had published recommendations for the prevention and control of COVID-19 for health care workers.7, 8 There is an enormous possibility that misconceptions among dentists could lead to the spread of infection in dental offices, thus, putting both the dentist’s and patient’s lives at risk. This necessitates rapid assessments of knowledge and perceptions of dentists regarding this new infection. In addition, we also aim to explore the role of different information sources and national lockdown in shaping their perceptions of COVID-19 during this global health crisis.
Materials and Methods
This is a web-based cross-sectional study conducted using a survey application (Google forms) to obtain responses from dentists all over India during the second week of April 2020. A self-constructed, structured questionnaire comprising of 22 questions among which four were open ended questions, was developed after reviewing pertinent literature and the international guidelines.9, 10, 11, 12 The developed draft survey instrument was distributed to ten randomly selected faculty members to assess its readability and validity before pretesting among 20 randomly selected dental professionals for clarity, relevance, and acceptability. Refinements were made as required to facilitate better comprehension before the final survey was distributed to the study population. The questionnaire was provided in English language. A convenient sampling method was used for data collection. Participants were classified on the basis of gender, age (24-35 years, 36-45 years, 46-55 years and >55 years), educational qualification (graduate, post-graduate students) and years of professional experience (<5 years, 5-10 years, 10-20 years, 20-30 years and >30 years). The time taken to complete the survey was approximately 5 minutes.
The 22-item questionnaire including socio-demographic details evaluated awareness of COVID-19, source of information, knowledge, different modes of transmission, precautions and risk prevention and perceptions regarding COVID-19. The participants were allowed adequate amount of time to read, comprehend, and answer all the questions. The information provided by each participant was maintained strictly confidential throughout the study by making the participants' information anonymous. Participation in this survey was voluntary and not compensated for. An informed consent (E-consent) was obtained from each participant prior to participation. The study was performed following the Helsinki Declaration as revised in 2013. The study was conducted following the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) guidelines.13
Statistical analysis
The data obtained were coded, validated, and analysed using statistical package for social sciences (SPSS) version 24 (IBM, Armonk, NY, USA). Descriptive analysis was applied to calculate the frequencies and proportions. The chi-square test was used to investigate the level of association among variables. The p-value was set at < 0.05 for statistical significance.
Results
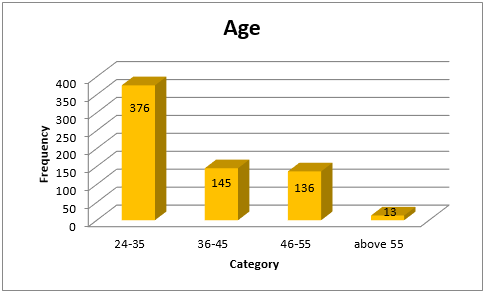
A total of 670 dental professionals participated in the survey, including 315 (47%) males and 355 (53%) females. Most of the participants belonged to the age group 24-35 years (56.1%) [Figure 1]. The majority of the respondents were post graduates (55.5%) and had less than 5 years of experience after graduation (42.1%). A good number of the dentists who participated were practising in the state of Kerala (77.3%). Almost all of the participants agreed to having heard of the novel corona virus (99.6%). According to majority of the participants, the primary sources of information about COVID-19 were social media, TV and newspapers with most participants relying on social media (37.2%).
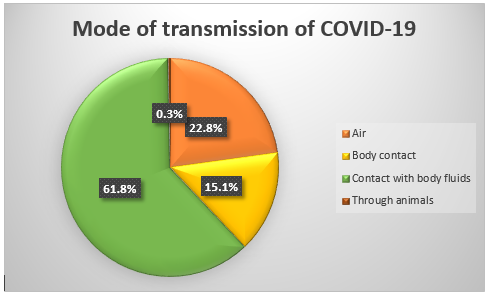
There is a significant difference between age categories in knowledge about source of origin of COVID-19 (p < 0.05) [Table 1]. Around 54% of the 24-35 age category respondents agree the origin of COVID-19 is viral genetic transformation. Here 61.8% of the respondents agree with the mode of transmission as contact with body fluids [Figure 2].
Table 1
Comparison between age and the knowledge about source of origin of COVID-19
Majority of the participants voted for carrying out only non-aerosol generating procedures as one of the protective measures during this time followed by safe distancing and use of PPEs. Approximately 70% respondents believe the incubation period of COVID-19 to be 14 days and 42% of those who say that belong to the 24-35 age category indicating a significant difference between the age categories regarding the knowledge of incubation period of COVID-19 (p < 0.05) [Table 2]. There also exists a significant difference between the years of experience in the field of dentistry and the knowledge of incubation period of COVID-19 (p < 0.05). Here 32% of the respondents with less than five years of experience believe the incubation period to be 14 days [Table 3]. No significant difference was observed between males and females regarding knowledge of incubation period of COVID-19 (p > 0.05).
Table 2
Comparison between age and the knowledge about incubation period of COVID-19
Table 3
Comparison between years of professional experience and the knowledge about incubation period of COVID-19
A good majority of the participants (79%) suspect a second round of viral spread with 94.6% of them anticipating a change in post lockdown practice including both a change in infection control procedures and a hike in service charges [Table 4].
Table 4
Proportion of participants expecting various changes in post lockdown practice
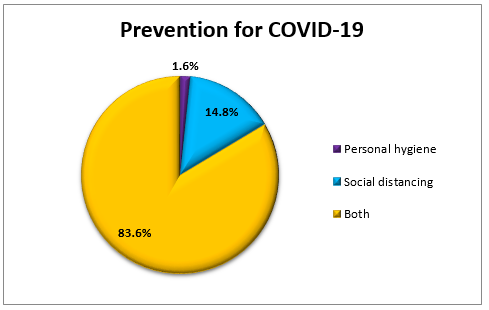
In addition, approximately 83% of the dentists felt that personal hygiene combined with social distancing could help to prevent COVID-19 transmission [Figure 3].
A considerable number of dental professionals refrained from practice during lockdown due to moral obligation towards society. Questions regarding COVID-19-related perceptions among dentists in the study were analysed separately using the chi-square test to examine their association with age and sex and across different categories of people. There is a significant difference between the male and female study populations with regard to mental health (p < 0.05) during the lock down period where around 59% of the males are relaxed and calm while around 33% of the females have fear of future [Table 5]. A significant difference in mental health was also observed between various age categories (p < 0.05) with around 47% of them in the 24-35 age category being relaxed and calm during the lock down period [Table 6]. It is also noteworthy that dental professionals all over India were able to engage themselves in various activities during the lockdown days with a good number among them being able to spend quality time with their families (73.4%).
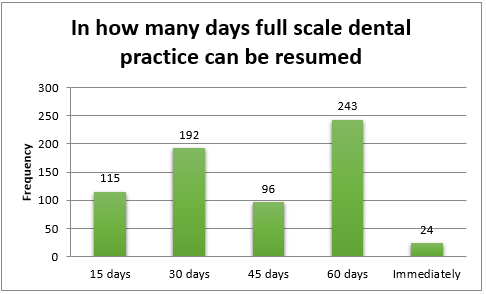
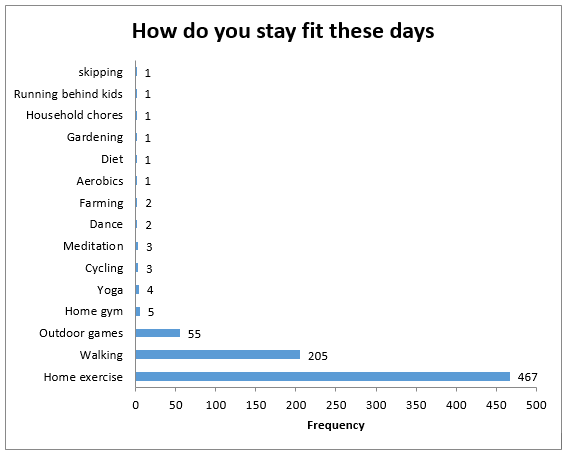
Majority of the participants expect to resume full scale dental practice within 60 days post lockdown [Figure 4]. When asked about the various means by which dentists are maintaining body fitness during these days most of them answered with home exercises [Figure 5].
Table 5
Comparison between gender and mental health during the lockdown period.
|
Gender |
Mental health in lockdown days |
Total |
Pearson Chi-Square |
p value |
||
|
Fear of future |
Relaxed and calm |
Stressed |
||||
|
Male |
95 |
187 |
33 |
315 |
7.166 |
0.028 (<0.05) |
|
Female |
120 |
178 |
57 |
355 |
||
|
Total |
215 |
365 |
90 |
670 |
||
Table 6
Comparison between age and mental health during the lockdown period.
Discussion
This survey aids us in gaining an insight into the level of awareness, knowledge and perception of Indian dentists on infection control with a special emphasis on COVID-19 outbreak in 2020 at the time of the national lockdown. Currently, COVID-19 is a global topic of discussion in the media and among the public, especially among health care workers and patients. With the currently mounting COVID-19 transmission causing apprehensions in everyone, including health officials and health systems, an important question arises regarding how we as dentists manage information to help out at this hour of public health crisis. The distance between the working field and the dentist is approx. 35–40 cm, and certain procedures can be very time-consuming, which puts the dentist at a higher risk of contracting COVID-19.9, 14 Knowledge and perceptions of the participants regarding COVID-19 varied among the different categories of age and also according to the years of experience in the field of dentistry.
Our study revealed that dentists in India are well aware of the emergence of novel corona virus pandemic. We also found that most of the respondents depended on social media, TV and newspapers primarily for accessing information about COVID-19. Relying on authentic sources for data related to COVID-19 is of prime importance for the preparedness and response of dentists due to the unfathomable diversity of information available on the Internet, including unverified malicious information that can spread quickly and mislead individuals. In particular, health authorities and scientists have warned that widespread misinformation about COVID-19 is a serious concern causing xenophobia worldwide.15, 16, 17, 18 The findings of this study suggest significant knowledge gaps between the dental professionals in India, particularly about the mode of transmission and incubation period of COVID-19. For instance, less than half (42%) of the participants aged 24-35 years agreed to an incubation period of 14 days for COVID-19. The estimated incubation period of COVID-19 is up to 14 days.5, 19 Dentists in this study varied in their knowledge about the incubation period of the disease, but being the key factor in determining the safe period to treat suspected patients, it is essential to know the right incubation period.20 However, it’s imperative for dentists to carry on with preventive measures for all their patients, all the time. Nonetheless, nearly 83% of the respondents believed that a combination of personal hygiene measures and social distancing is effective in preventing COVID-19. A vast majority of them strongly agreed that carrying out non-aerosol generating procedures in the dental office is of utmost importance.
The recent national lockdown in India in connection with the global outbreak of COVID-19 has definitely had its impact on the mental health of the masses. This is particularly applicable to the dental society as they have been included in the high risk categories with 33% of the female dentists under study expressing concerns regarding the uncertainty that prevails. Our study revealed a significant difference in the mental state of dentists between males and females. On the other hand, this also gave an opportunity for many of them to plan ahead the changes to be introduced in their post lockdown practice to combat such situations effectively with the improvement in infection control measures being given the topmost priority. Furthermore, dentists being known for their hectic professional schedule were able to use this period to their benefit by indulging themselves in more productive activities and by spending quality time with their families. This could also be the chief reason for the more relaxed and calm nature of the male dentists under study. This time could also be utilized effectively by young dentists to expand their knowledge and to prepare for upcoming exams being that time of the year. So, a larger part of the study population being postgraduates and therefore likely to fall in the 24-35 age category could be the reason for the increasingly relaxed mental state among them.
A good part of the questionnaire was limited to closed-ended questions to reduce information bias. Nevertheless, it is important to stress that this survey had some limitations that need to be addressed, including the relatively low response rate, which resulted in a smaller than expected sample size. This could have been due to the short period of data collection. However, we did manage to obtain a moderate sample size. Moreover, this could also be attributed to the fact that the recent COVID-19 outbreak might have caused many to get engrossed in watching the news and taking care of personal affairs paving way to selection bias and sampling errors, thus, making it difficult to generalize our results. In addition, the data presented in this study are self-reported and partly dependent on the participants' honesty and recall ability; thus, they may be subject to recall bias. Finally, due to the 40 day national lockdown in India that involved the closure of higher educational institutions during the COVID-19 outbreak, the institutional review board could not be approached. Despite these limitations, we cannot overlook the valuable information regarding the knowledge and perceptions of dental professionals in India, which this survey has furnished us with during the most testing times the world has witnessed recently in relation to a pandemic.
Conclusion
Our survey unveiled a significant gap in the knowledge levels, and discrepancies in perceptions of COVID-19 among our study participants. As the global threat of COVID-19 continues unabated, there lies a greater responsibility with the dental professionals in India to educate themselves and the general population regarding the risks and preventive measures of COVID-19. Be that as it may, the current global scenario undeniably puts our technological advancements and scientific accomplishments to test. This warrants further research on the topic so that we may become better equipped to fight off these microorganisms that threaten the very existence of human species.