Introduction
Good knowledge of the internal anatomy of the teeth and its variations is imperative to ensure a favourable outcome of endodontic treatment. The root canal anatomy of the maxillary first molar has been extensively reviewed in the literature, revealing that this tooth may present a great variation1 in root canal configurations, mainly in the mesiobuccal canal. Cleghorn et al. investigated that the root canal anatomy of maxillary first molars and found that about 57% of mesiobuccal root, have more than two root canals (60.5% in laboratory studies and 54.7% in clinical studies), whereas majority of distobuccal and palatal roots had a single canal (98.3% and 99.0%, respectively).2 Mesiobuccal root of maxillary 1st molar contains a two root canal system than a single canal, and the incidence of second canal i.e. mesiobuccal 2 canal has been reported in between 18.6% and 96.1%, whereas distobuccal canal 2 has been reported in between 1.6% and 9.5%, and incidence of two root canals in the palatal root has been reported in between 0.2% to 7.0%. Few cases have reported presence of three canals in the mesiobuccal roots Kumar R, Badole GP et al,3 Kaushik M et al,4 Kakkar P et al.4, 5, 6. Two such clinical studies has reported their incidence to be 1.% to 10%7, 8 Kottoor et al. in 2010 have reported 7 canals in maxillary 1st molar (3 mesiobuccal canls, 2 distobuccal and 2 palatal) whereas in 2011 he reported 8 canals orifices using cbct (3 mesiobuccal .3 distobuccal and 2 palatal).
Acosta and Trugeda first documented 3 root canals in a single Mesiobuccal Root.9 In previous case report, they have described the incidence of second mesiobuccal canal as vertucci type 2 (i.e. 2-1) which was found to be 42% in males and 37% in females. Vertucci type 4(i.e. 2) was also present in 29% of males and 27% of females. However, the prevalence of an Mesiobuccal3 canal is present rarely. According to Vertucci type 8(i.e. 3) the total prevalence in males and females was found to be 0%. However, Sert and Bayirli classified further where in type XVII (i.e. 1-3-1) and type XVIII (i.e. 3-1) was reported 1% and 0% in females respectively.7
Nowadays, technological advances have been developed, and different techniques have been introduced to simplify the assessment of variations in root canal anatomy. For this purpose, dental operating microscope and Cone Beam Computed Tomography have been proven to be superior over the traditional diagnostic tools used till now. Cone Beam Computed Tomography assists the practitioner to identify root canal anatomy, number of canals, and relative positioning even in the presence of calcific metamorphosis and dystrophic calcifications.9
This article presents a case report with incidence of three canal orifices in mesiobuccal root of maxillary 1st molar. The purpose of this case report is to highlight the importance of having thorough knowledge of the complex root canal anatomy.

Case Report 1
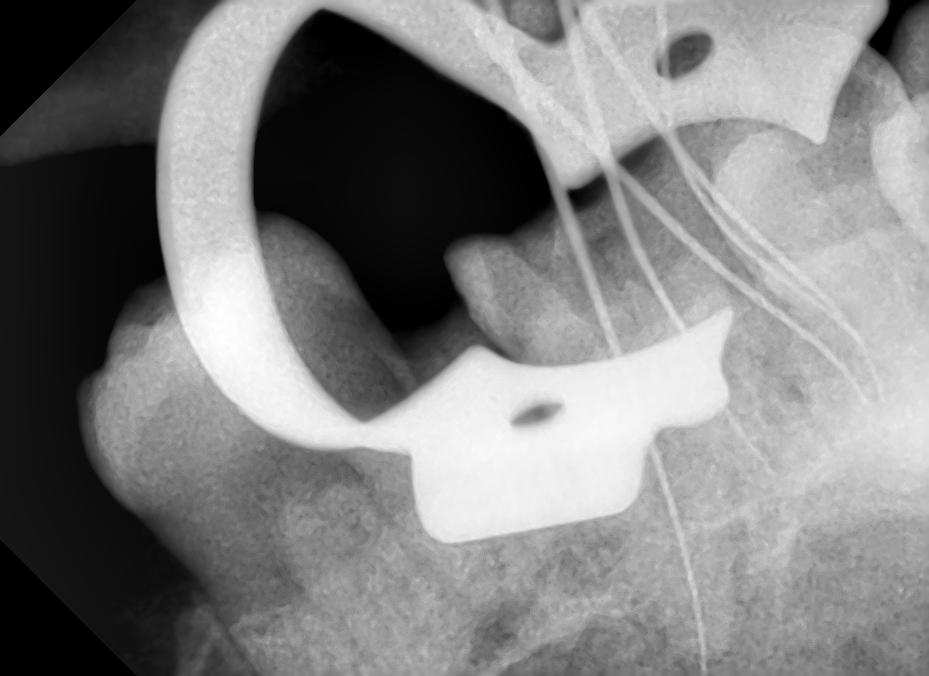
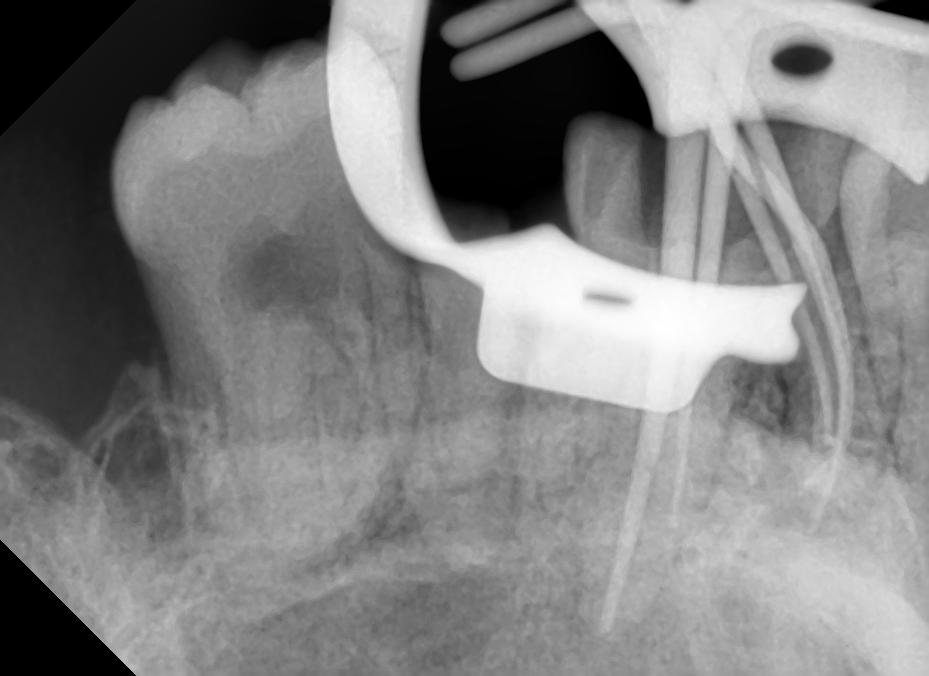
A 25-year-old male was referred to the department of conservative dentistry and endodontics, Rural Dental College Loni for treatment of maxillary left first molar. Patient came with the complain of pain since a week, which was continuous and dull in nature. Clinical examination revealed deep disto-occlusal caries. There was tenderness on percussion and palpation and delayed response to cold pulp testing. Radiographic interpretation revealed a radiolucent area involving enamel, dentin and approaching pulp. Periapically loss of lamina dura was seen with respect to distal root. After clinical and radiographic examination confirm diagnosis of chronic irreversible pulpitis and acute apical periodontitis and endodontic treatment was planned.
LA was administered using 2% Lignocaine (Lox 2%, Neon Lab Ltd., Mumbai, Maharashtra, India), posterior superior alveolar nerve block technique was given on the left side. Under rubberdam isolation access cavity was prepared (Figure 3). Under 3.5x magnification using surgical loupes the anatomy of 26 was identified. It presented as 3 canal orifices in Mesiobuccal root, 1 canal orifice in distobuccal and palatal root.) Working length was checked with ISO size #10k file (mani, JAPAN) using an electronic apex locator (Root ZX III, J Morita, Tokyo, Japan). Shaping and cleaning was done using Crown down technique till ISO tip size mb1=mb2=mb3= 25.04% db=25.06% and p=30.06% (Micromega Hero gold rotary files). Copious irrigation was done with 10ml of 5% NaOCL followed by normal saline and 17% EDTA. Final irrigant was normal saline. Master cone was checked using intraoral periapical radiograph. All the canals were dried by placing paper points till working length. Obturation was done with Iso size #0.4% and 0.6% Gutta percha points by using AH plus sealer and lateral condensation technique.



Discussion
Root canal anatomy of the teeth is a very complex system which comprises of a number of foramina which open at different locations - lateral, collateral, accessory, etc.10
Disinfection in such systems is a challenging task. Shaping and cleaning of maxillary first molar tooth, especially with respect to the MB root, may be difficult.
The current case report present case of three MB canals in single MB root of maxillary first molars. There is a difference in the literature with the terminology used to describe additional canals in the Mesiobuccal root of maxillary molars such as Baratto Filho et al., 2009 described the terminology MB1, MB2, and MB3 canals, Acosta Vigouroux and TrugedaBosaans, 1978 described MB, collateral MB and second collateral, while Favieri et al., 2006 gave MB1, MB2, and MP canals to avoid this misperception, Karthikeyan and Mahalaxmi proposed the terminology of additional canals in a single root starting from the most buccal canal and heading in a platal direction. Therefore, the three canals in the Mesiobuccal root are denoted as Mesiobuccal(MB), Second Mesiobuccal(SMB), and Mesiobucco palatal(MBP).11
In the present case, visual examination of the pulpal floor under magnification (3.5x) using surgical loupesand search of bleeding points with the DG16(Dudley Glick) indicated presence of additional canals orifices. Bleeding points of both Mesiobuccal2 and Mesiobuccal 3 was noted at 1 mm interval from MB1 canal palatally. In this case root canal anatomy of mesio buccal root showed (3-1) configuration i.e. type XVIII Sert and Bayirlis classification of additional canals to vertucci’s classification in which three canal orifices joint apically and terminate as single canal.
In the maxillary molars, complex root canal anatomy are not uncommon, with the number of canals ranging from 1 to 8. Vertucci identified eight different types of root canal configurations. Recently, Sert and Bayirli have proposed 14 new additional canal configuration which highlights the complexity of root canal system.
Radiographic assessment is one of the vital constituents in diagnosing the endodontic problems and also to predict the root canal morphology to some extent.10
.
Conclusion
This Case report shows that the clinician must have through knowledge of complex root canal anatomy for proper diagnosis and treatment planning. This enables the clinician to overcome possible challenges of vivid canal configrations and achieve successful three dimensional obturation.
The frequency of maxillary first molars with three Mesiobuccal canals is very rare. However, each case should be investigated carefully, clinically and radiographically, to detect distinctive anatomic aberrations.