Introduction
Natal and neonatal teeth are rare dental anomalies involving the disturbances in the biological chronology of teeth and often linked with diverse superstitions among different ethnic groups. Teeth existing in the oral cavity at the time of birth are referred to as natal teeth, and teeth that erupt within 30 days of life are termed as neonatal teeth. The aetiology of occurrence of these natal or neonatal teeth is still not established and usually associated with a series of contributing potential risk factors such as infection or malnutrition, febrile states, superficial position of tooth germs, hormonal stimulation, heredity, hypovitaminosis, osteoblastic activity or trauma. Generally, such teeth are found to be located in the same position as that of the primary teeth and more commonly in the incisor and molar regions of the lower arch. Their prevalence is considered to be low, ranging from 1:1000 to 1:30,000 live births. These teeth are more frequently seen in females than males and mostly reported in pairs in 38% to 76% of infants.1, 2, 3, 4, 5
In 90% of reported cases, natal and neonatal teeth are found to be prematurely erupted primary teeth, whereas, in less than 10% of situations, they are supernumerary teeth. Natal or neonatal tooth may appear like a normal primary tooth but in most of the cases, the crown is small and conical in shape that may appear brownish-yellow in colour due to associated enamel and dentin hypoplasia. Roots are poorly formed and ill-defined, which are barely attached to the alveolar mucosa by a thin flap of soft tissue. Besides, they may be associated with hypoplasia of the enamel and dentin and appear brownish-yellow in colour.3, 4, 6, 7
Since the natal and neonatal teeth have typical clinical manifestations and are associated with various risks, quite obviously they attract the interest of the parents and dentists. Infants with prematurely erupted teeth must be immediately referred to the Paediatric Dentist for a detailed examination to establish the appropriate diagnosis and for further treatment planning and management of the case.
This article presents a series of 3 cases of Natal teeth and their dental management.
Case Report 1
A 28-days-old female infant was referred to the Department of Pediatric and Preventive Dentistry, Jamia Millia Islamia, New Delhi, India with a chief complaint of a tooth present in the lower front region of the jaw since birth.
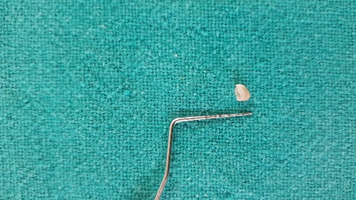
The intraoral examination revealed the presence of a calcified structure in the anterior mandibular region. The structure was similar to primary mandibular incisor in many aspects and was poorly calcified. It was loosely attached to the alveolar ridge and was extremely mobile and the mucosa around the tooth was inflamed (Figure 1, Figure 2). A radiograph was not possible and a diagnosis of a natal tooth was confirmed based on the clinical presentation. Besides, no clinical signs and symptoms of any systemic illness, congenital anomalies, or syndromic involvement were observed in the infant during the examination.
Figure 1
Photograph showing clinical appearance of a single natal tooth in primary mandibular central incisor region

The extraction of a natal tooth was planned as it was mobile and causing discomfort to the mother while nursing. A complete hemogram was found to be satisfactory and the patient had already taken Vitamin K supplement at birth. Extraction was carried out using 2% lignocaine with adrenaline local infiltration technique after the application of topical anaesthesia followed by the curettage of the extraction site (Figure 3). Postoperative haemostasis was achieved and post-extraction instructions were given. The patient was recalled after 5 days for post-operative evaluation and the healing was found to be uneventful.

Case Report 2
A 3 weeks old female infant was referred to the Department of Pediatric and Preventive Dentistry, Jamia Millia Islamia, New Delhi, India with a chief complaint of the presence of a calcified mass in the lower jaw since birth. Although the mother reported no discomfort while feeding but the grandparents did not consider the occurrence of such tooth to be lucky and insisted on immediate extraction. On intraoral examination, a tooth-like crown structure was observed in the 81 region with grade II mobility on palpation. Ulceration on the ventral surface of the tongue was also observed (Figure 4, Figure 5). The radiographic examination of the child was not possible, a diagnosis of a natal tooth was confirmed based on the clinical presentation and extraction was planned following the satisfactory blood investigations reports.
Figure 4
Photograph showing clinical appearance of a single natal tooth in primary mandibular central incisor region

Extraction was carried out under local anaesthesia with 2% lignocaine with adrenaline after application of topical anaesthesia and careful curettage of the extraction socket was done to remove any cellular remnants of the natal tooth (Figure 6). The parents were given instructions about postoperative care and a recall visit after 3-4days later was scheduled.


Case Report 3
A 5-days-old male child was referred to the Department of Pediatric Dentistry, Jamia Millia Islamia, New Delhi, India with a chief complaint of teeth present in the lower front region of the jaw since birth. Medical history revealed the infant was born full-term; normal delivery with no complications.
Oral examination revealed two premature teeth in the 71 and 81 regions (Figure 7), whitish opaque in colour, and both of them exhibiting grade II mobility. Clinically, the crown size of the tooth present on the right side was smaller compared to the left one, and all the edges were smooth; the gingiva was of normal appearance. There was no evidence of any ulcerations on the tongue or gingiva of the infant (Figure 7). The mother did not complain of any feeding difficulties but was concerned by the premature occurrence of the teeth.
A radiograph was taken, that revealed two calcified conical structures, not belonging to the normal series of primary dentition (Figure 8). The final diagnosis of natal teeth was made and extraction was considered as the treatment of choice. Following the satisfactory blood investigations reports, extraction was carried out under local anaesthesia with 2% lignocaine with adrenaline after application of topical anaesthesia (Figure 9) and careful curettage was done to eradicate the remaining teeth remnants from the socket. The mother was advised about the postoperative care and was asked to report for a recall visit after a few days.


Discussion
Frequently the natal teeth are prematurely erupted deciduous teeth and should be preserved excepting those interfering with nursing or resulting in ulceration of the infant’s tongue causing any grave complication or causing injury to the mother’s breast while suckling. A major complication from the natal tooth is Riga-Fede-Disease when the continuous trauma by the sharp incisal edges results in the ulceration on the ventral surface of the tongue.8, 9 Usually, the treatment of natal and neonatal teeth includes grinding of the sharp edges of the tooth structure, fabrication of composite breastfeeding splint, and extraction. Many authors recommend their extraction as soon as they are visible in the oral cavity since there are higher chances of an infection following an injury to attachment tissue and subsequently greater risk of tooth aspiration by the infant when it exfoliates.1, 3, 10, 11
The extraction should be performed with the appropriate considerations of prophylactic administration of vitamin K as the coagulation mechanism in infants is not fully developed.2, 12 Complications after extraction are rare but some authors have reported the recurrence of a natal or neonatal tooth or continued growth of the root.3 Sometimes, after the extraction of natal or neonatal teeth, the root persists to develop in the socket which may demand further treatment.3, 13, 14 King and Lee (1989)15 reported only 9.1% of infants with natal and neonatal teeth developing residual teeth following the exfoliation or extraction of these teeth. Similarly, Kaur G, et al. (2019)3 reported the development of residual neonatal following the natural exfoliation of neonatal teeth in a preterm infant.
Residual tooth formation is not experienced in most of the situations after the extraction, still, there is an involvement of the risk and the parents should be well informed and motivated for the regular dental check-ups.
Conclusion
Infants with natal teeth must be carefully examined for their diagnosis and treatment planning. The decision to retain or extract them should be evaluated clinically as well as radiographically. It is necessary to differentiate supernumerary teeth and teeth of primary dentition, the latter one should be preserved and maintained in healthy conditions. However, prematurely erupted teeth with mobility should be extracted to prevent aspiration while nursing. The clinician should consider the complete hemogram, vitamin K profile, and the overall wellbeing of the infant before extracting such teeth to prevent the risk associated with hypoprothrombinaemia. Periodic follow-ups should be scheduled to avoid complications and to evaluate recurrences.