- Visibility 445 Views
- Downloads 38 Downloads
- Permissions
- DOI 10.18231/j.ijohd.2021.033
-
CrossMark

Silver diamine fluoride for early childhood caries- A boon for dentists during COVID-19 pandemic
Abstract
Early Childhood Dental Caries (ECC) is a global burden. Management protocols of a disease are changing constantly with the improving knowledge of the disease, new materials, and treatment strategies. Clinical studies have confirmed the use of Silver Diamine Fluoride (SDF) is an effective and efficient caries arrest and a prevention therapy. It is a simple, safe, and quick treatment option for carious deciduous teeth. More importantly, caries removal is not indicated before the application which makes the topical application of SDF solution a good alternative in the management of ECC during the backdrop of the Covid-19 pandemic.
Introduction
Early childhood caries is one of the most prevalent chronic childhood diseases worldwide. More than 532 million children worldwide are affected by dental caries of primary teeth, and it is frequently observed in unprivileged groups in developing countries.[1], [2] Although, dental caries is a preventable and controllable oral disease, still a great burden had to been put on curative care. The prevalence of untreated cases of dental caries in young children remains a deep-rooted challenge. It may be because standard dental therapies for caries are either beyond reach or unaffordable to most of the pediatric population.[2]
Even though, fluoride application is considered as a well-established primary preventive measure, several children present with deep carious lesions which involve deeper part of the dentine. These teeth need removal of carious tissues using rotary instruments or manual excavation followed by restoration which results unpleasant dental experience in pediatric patients. Extensive tissue loss may lead to dislodgement of restorations, repeated infection, and indirect restorations. Apart from that, management of uncooperative pediatric patients may demand lengthy treatment sessions or advanced forms of behavior management such as sedation or general anesthesia. These are essentially posed burden to dental units, especially in developing countries.[3]
The Covid-19 is a highly contagious viral disease which has become a huge burden globally since 2019. It is a disease caused by the pathogen, Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2).[4] On January 31, 2020, the World Health Organization (WHO) announced that the Covid-19 outbreak had become a public health emergency of international concern. Later, it was categorized as a pandemic on March 11, 2020.[5]
According to the scientific evidence, interpersonal transmission is possible via infected respiratory droplets by direct or indirect contact with nasal, conjunctival, or oral mucosa, when respiratory particles are inhaled or deposited on these mucous membranes.[6] Emerging evidence of the airborne risk of Covid- 19 virus should also be taken into consideration.[7]
The Covid-19 pandemic has shaken the global healthcare structure and oral healthcare has been no exception. The World Health Organization (WHO), the Centers for Disease Control and Prevention (CDC) guidance on oral health services, and the Cochrane community recommended delaying routine dental care. Around 60.8%, 35.5% and 18.3% of preschool aged children in Wuhan, China had self-reported dental cavities, toothache, and halitosis, respectively.[8] Most of the people who suffered with dental problems did not visit dental clinics due to limited dental services during the pandemic and fear of contracting the Covid-19 virus through dental care.[9]
Alternative measures had been discussed in the literature to offer dental assistance during these unusual times, such as teledentistry, online visits and over the phone advice.[10], [11] Non / low aerosol generating procedures are good alternatives for caries management in midst of Covid 19. Use of SDF is an efficacious and safe approach especially for pediatric patients in both pandemic and post pandemic period.
Efficacy of SDF in dental caries prevention and arrest
Silver diamine fluoride (SDF) is a clear liquid containing silver, fluoride and ammonia complex that has been identified as a promising therapeutic agent against dental caries in both primary and permanent dentition.[2], [3], [4], [5], [6], [7], [8], [9], [10], [11], [12], [13] It combines the antibacterial effects of silver and the remineralizing effects of fluoride, which makes the SDF a good treatment option for managing caries lesions.[12] In-vitro studies showed significantly less number of S. mutans and L. acidophilus within the lesions treated by local application of SDF, supporting the fact that SDF possessed an anti-microbial activity against cariogenic bacteria.[14], [15]



Further, studies demonstrated the ability of SDF to slow down the demineralization process of dentine by preventing collagen degradation by inhibiting Matrix metalloproteinases and cathepsins.[15], [16], [17] Many clinicians working on caries prevention therapies have presented steady findings and emphasized that SDF is surely more potent than the fluoride varnishes in arresting dental lesions with no reported evidence of pulpal damage post application.[2]
Most of the clinical studies in literature used 38% of SDF solution and it is the recommended strength of SDF to be used to achieve better results.[13], [14], [15], [16], [17], [18] The clinical effectiveness of 38% SDF solution in arresting dental caries of primary teeth and preventing and arresting root caries in adults has been consistently supported by all of the systematic reviews.[19], [20], [21] As stated by Gao et al. in 2016, the overall proportion of arrested dental caries following SDF treatment was 81% (95% CI, 68% to 89%; P < 0.001).[20] SDF application on carious primary teeth shows promising results in arresting and preventing of caries when compared with use of fluoride varnish. A prospected controlled clinical trial carried out by chu et al. in 2002, showed that an annual application of 38% SDF was more effective than 3 month application of 5% NaF varnish in arresting dentinal caries of primary teeth. Results of this study agree with observations of many other studies.[22], [23], [24]
A randomized controlled study by dos Santos Jr VE et al. compared the efficacy of 30% SDF with of Glass Ionomer Cement (GIC) when used as an intermediate restorative technique (IRT) and found that SDF was 1.73 times more effective in arresting caries than IRT.[25]
Contraindications and considerations for SDF use
SDF had been used for over 80 years with no serious complications.[18] However, use of SDF is contraindicated in patients with silver allergy, clinical/ radiographic signs, or symptoms of periapical pathology and significant desquamative gingivitis or stomatitis.[26], [27] Black discoloration of the lesions, staining every surface it contacts and temporary metallic taste are the commonly claimed side effects of SDF application. Even though some studies supported use of Potassium Iodide (KI) with SDF to reduce the discoloration, insufficient evidence exists to conclude positive clinical results.[28] Despite the advantages, use of SDF will be less popular in dental practice due to compromised esthetic. However, literature reports poorer parental acceptance for use of SDF in anterior teeth compared to posterior teeth.[29], [30], [31], [32] Sultan A et al. (2020) reported that parental acceptance was significantly less for teeth located in esthetic zones such as maxillary incisors and in children below three years of age.[29] But the willingness of parents for SDF was increased with the level of uncooperativeness of the child.[29], [30], [31], [32], [33] An umbrella review done by Sabbhag et al. on 2020, stated that pre-operative instructions could significantly improve parental acceptance of SDF application.[32] The average lethal dose of SDF by oral and subcutaneous administration was 520 mg/kg and 380 mg/kg, respectively. One drop of 38% SDF liquid contains 9.5 mg silver diamine fluoride. One drop of material is sufficient to treat up to five teeth.[34] The recommended dosage is one drop (25 μL) of 38% SDF liquid per 10 kg of body weight child per treatment visit.[34]
Protocols and Application
Frequency of application
Annual and semiannual applications have been studied in clinical trials and six-monthly application was found to be more effective than annual application.[35], [36]
Clinical Technique
Preparation
Cover the work-surfaces with plastic wraps to avoid stains due to SDF and use plastic bibs for the patient.
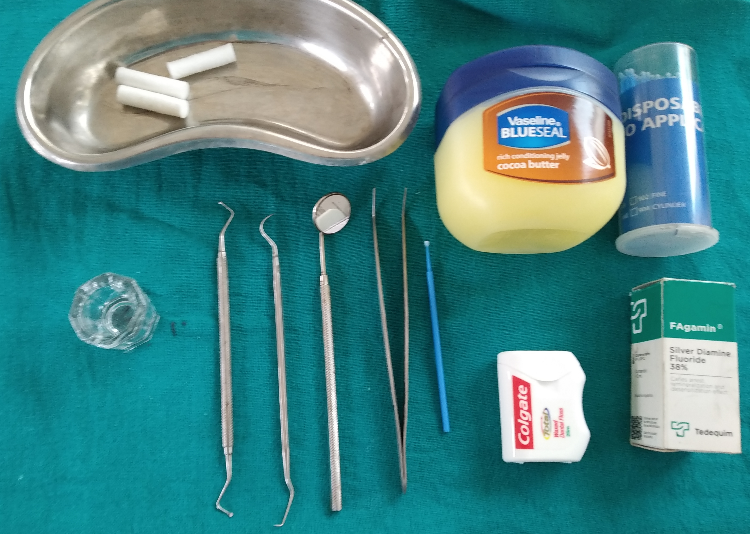
Take precautions to minimize unwanted side effects. Use maximum isolation with rubber dam or if is not possible due to poor cooperation, cotton wool rolls and gauze can be utilized. Application of petroleum gel around the lips and vermillion borders will reduce the risk of staining. [[Figure 1]]
Caries removal
Removal of carious tissue is not indicated prior to application of SDF as it does not show added advantage in caries arrest.[37] However, removal of gross debris from cavities will allow better SDF contact with denatured dentin and removal of infected dentine will sufficiently reduce the bacterial load.[18]
Application of SDF
SDF solution (38%) should be applied directly over the dried carious lesions using a micro brush. Minimum but adequate amount of the solution is used cautiously to prevent inadvertent gingival discoloration. No more than one drop of 38% SDF solution is recommended in one visit. [[Figure 2]] [[Figure 3]] It is ideally recommended to remove the excess SDF using cotton pellets/ gauze, after leaving one to three minutes in contact.[34]
Follow-up
Follow up visit is recommended after 2-4 weeks of the first application of SDF to check the efficacy of the procedure done. [[Figure 4]] If the lesions do not show features of an arrested site (Dark brown color, hard texture), reapplication is indicated.[38]
Restorations after SDF therapy?
SDF therapy is proven to arrest dentin caries and it results a black deposit on the treated site which may cause an esthetic concern of both parents and the child. A tooth-colored restoration can mask the stains caused by SDF- arrested dentine caries and recontour the tooth into functional shape. Placement of GIC restoration on SDF treated, arrested lesions, following the concept of ART improved parental satisfaction significantly.[39] Previous application of SDF does not show an influence on bonding strength between GIC and the dentine.[40] SDF is a valuable option of non-surgical caries management in is COVID-19 era.
Dental clinics carry a high risk of cross infection due to the nature of dental treatment and it is critical for the Covid-19 because of the aerosol generating dental treatment procedures. So, routine dental treatments and elective procedures were suspended across the world during this period. This in turn has caused an upturn in the numbers of children suffering from dental caries. Dental professionals around the world are confronting the consequences of disrupted oral health care during the pandemic. There are many reasons for this including lack of access to care, or a personal decision to forgo care due to fear of contracting the infection in the dental office, or lack of focus on home oral care due to altered diet patterns, sleeping patterns and limited affordability or availability of oral hygiene products during the pandemic. Since caries removal is not necessary during treatment with SDF, it accounts under non-aerosol generating dental procedure. Yet, it gives good clinical results in caries arrest and prevention. Application of SDF is a simple procedure that keeps the treatment session short, even with less cooperative pediatric patients.[24], [25], [26] Furthermore, guidelines and recommendations on Covid-19 global pandemic induced dental practice modifications pertaining to pediatric dentistry highlighted the importance of using SDF underpinned minimally invasive dental practice to mitigate infection transmission by aerosol generation.
Conclusion
Use of SDF is a better principal that can be practiced enhancing prevention and minimal operative intervention. More importantly, it is a child friendly, cost effective and successful management strategy. SDF application could be carried out with minimum facilities. Therefore, promoting the use of SDF is an effective treatment mode particularly during a pandemic such as Covid-19.
Source of Funding
None.
Conflict of Interest
None.
References
- Bernabe E, Marcenes W, Hernandez CR, Bailey J, Abreu LG, Alipour V. Global, regional, and national levels and trends in burden of oral conditions from 1990 to 2017: a systematic analysis for the global burden of disease 2017 study. J Dent Res . 2020;99(4):362-73. [Google Scholar] [Crossref]
- Sultan A, Juneja A, Siddiqui M, Kaur G. Silver diamine fluoride as a proactive anti-caries tool: A review. Int J Oral Health Dent. 2019;5(2):63-71. [Google Scholar] [Crossref]
- Yee R, Sheiham A. The burden of restorative dental treatment for children in Third World countries. Int Dent J. 2002;52(1):1-9. [Google Scholar]
- Adhikari SP, Meng S, Wu YJ, Mao YP, Ye RX, Wang QZ. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect Dis Poverty. 2020;9(1):1-12. [Google Scholar] [Crossref]
- . World Health Organization (WHO). Timeline of WHO’s response to COVID-19.. . 2020. [Google Scholar]
- Cevik M, Kuppalli K, Kindrachuk J, Peiris M. Virology, transmission, and pathogenesis of SARS-CoV-2. BMJ. 2020;371:1-6. [Google Scholar] [Crossref]
- Carducci A, Federigi I, Verani M. Covid-19 airborne transmission and its prevention: Waiting for evidence or applying the precautionary principle? Atmosphere (Basel). Atmosphere. 2020;11(7). [Google Scholar] [Crossref]
- Liu C, Zhang S, Zhang C, Tai B, Jiang H, Du M. The impact of coronavirus lockdown on oral healthcare and its associated issues of pre-schoolers in China: an online cross-sectional survey.. BMC Oral Health. 2021;21(54):1-6. [Google Scholar] [Crossref]
- Pasiga BD. Relationship knowledge transmission of covid-19 and fear of dental care during pandemic in South Sulawesi, Indonesia. Pesqui Bras Odontopediatria Clin Integr. Pesquisa Bras Odontopediatria Clín Integrada . 2020;21:1-12. [Google Scholar] [Crossref]
- Shamsoddin E, Detora LM, Palone MRT, Bierer BE. Dental Care in Times of the COVID-19 Pandemic: A Review. Med Sci. 2021;9(1):1-13. [Google Scholar] [Crossref]
- Ghai S. Teledentistry during COVID-19 pandemic. Diabetes Metab Syndr. 2020;14(5):933-8. [Google Scholar] [Crossref]
- Crystal YO, Niederman R. Evidence-based dentistry update on silver diamine fluoride. . Dent Clin. 2019;63(1):45-68. [Google Scholar] [Crossref]
- Chu CH, Lo EC. Promoting caries arrest in children with silver diamine fluoride: a review. . Oral health Prev Dent. 2008;6(4):315-21. [Google Scholar] [Crossref]
- Knight GM, Mcintyre JM, Craig GG, Zilm PS, Gully NJ. An in vitro model to measure the effect of a silver fluoride and potassium iodide treatment on the permeability of demineralized dentine to Streptococcus mutans. Aust Dent J. 2005;50(4):242-7. [Google Scholar] [Crossref]
- Mei ML, Chu CH, Low KH, Che CM, Lo EC. Caries arresting effect of silver diamine fluoride on dentine carious lesion with S. mutans and L. acidophilus dual-species cariogenic biofilm. . Med Oral Patol Oral Cir Bucal . 2013;18(6):824-31. [Google Scholar] [Crossref]
- Mei ML, Ito L, Cao Y, Li QL, Chu CH, Lo E. The inhibitory effects of silver diamine fluorides on cysteine cathepsins. J Dent. 2014;42(3):329-64. [Google Scholar] [Crossref]
- Mei ML, Ito L, Cao Y, Li QL, Chu CH, Lo E. The inhibitory effects of silver diamine fluorides on cysteine cathepsins. J Dent. 2014;42(3):329-35. [Google Scholar] [Crossref]
- Cohen JG, Greenwall L, Barry S. Silver diamine fluoride - an overview of the literature and current clinical techniques. Br Dent J. 2020;228(11):831-8. [Google Scholar]
- Clemens J, Gold J, Chaffin J. Effect and acceptance of silver diamine fluoride treatment on dental caries in primary teeth. J Public Health Dent. 2018;78(1):63-8. [Google Scholar] [Crossref]
- Gao SS, Zhao IS, Hiraishi N, Duangthip D, Mei ML, Lo EC. Clinical trials of silver diamine fluoride in arresting caries among children: a systematic review. JDR Clin Transl Res. 2016;1(3):201-11. [Google Scholar] [Crossref]
- Seifo N, Robertson M, Maclean J, Blain K, Grosse S, Milne R. The use of SDF in dental practice. Br Dent J . 2020;228(2):75-81. [Google Scholar] [Crossref]
- Chu CH, Lo E, Lin HC. Effectiveness of Silver Diamine Fluoride and Sodium Fluoride Varnish in Arresting Dentin Caries in Chinese Pre-school Children. J Dent Res. 2002;81(11):767-70. [Google Scholar] [Crossref]
- Duangthip D, Wong M, Chu CH, Lo E. Caries arrest by topical fluorides in preschool children: 30-month results. J Dent. 2018;70:74-9. [Google Scholar] [Crossref]
- Trieu A, Mohamed A, Lynch E. Silver diamine fluoride versus sodium fluoride for arresting dentine caries in children: a systematic review and meta-analysis. Sci Rep. 2019;9(1):1-9. [Google Scholar] [Crossref]
- Santos V, Vasconcelos F, Rosenblatt A, Ribeiro AG. Paradigm shift in the effective treatment of caries in schoolchildren at risk. Int Dent J. 2012;62(1):47-51. [Google Scholar] [Crossref]
- Jeremy A, Horst H. UCSF Silver Caries Arrest Committee PMM. USCF Protocol for Silver Diamine Fluoride. Physiol Behav. 2016;176(3):139-87. [Google Scholar]
- SJL, Arangannal P, Jeevarathan J, SA. When and Where to use and not to use SDF ? - overview. Eur J Mol Clin Med. 2020;7(2):6567-72. [Google Scholar]
- Roberts A, Bradley J, Merkley S, Pachal T, Gopal JV, Sharma D. Does potassium iodide application following silver diamine fluoride reduce staining of tooth? A systematic review. Aust Dent J. 2020;65(2):109-26. [Google Scholar] [Crossref]
- Sultan A, Mehta A, Juneja A, Siddiqui M. Evaluating parental acceptance for silver diamine fluoride therapy - A pilot study. S Brazi Dent J RSBO. 2020;17(2):226-9. [Google Scholar]
- Crystal YO, Janal MN, Hamilton DS, Niederman R. Parental perceptions and acceptance of silver diamine fluoride staining. . J AM Dent Assoc. 2017;148(7):510-8. [Google Scholar] [Crossref]
- Bagher SM, Sabbagh HJ, Aljohani SM, Alharbi G, Aldajani M, Elkhodary H. Parental acceptance of the utilization of silver diamine fluoride on their child’s primary and permanent teeth. . Patient Prefer Adherence. 2019;13:829-35. [Google Scholar] [Crossref]
- Sabbagh H, Othman M, Khogeer L, Harbi HA, Harthi A. Abdulgader Yaseen Abdulgader A. Parental acceptance of silver Diamine fluoride application on primary dentition: A systematic review and meta-analysis. BMC Oral Health. 2020;20(1). [Google Scholar] [Crossref]
- Shivasharan PR, Jawdekar AM, Pankey NN, Unnikrishnan S. Acceptance of parents to silver diamine fluoride in pre-cooperative children: a cross-sectional study. J S Asian Assoc Pediatr Dent. 2019;2(2):49-55. [Google Scholar] [Crossref]
- Horst JA, Ellenikiotis H, Milgrom PM. UCSF Silver Caries Arrest Committee. UCSF protocol for caries arrest using silver diamine fluoride: rationale, indications, and consent. J Calif Dent Assoc. 2016;44(1):16-28. [Google Scholar]
- Zhi QH, Lo EC, Lin HC. Randomized clinical trial on effectiveness of silver diamine fluoride and glass ionomer in arresting dentine caries in preschool children. J Dent. 2012;40(11):962-9. [Google Scholar] [Crossref]
- Fung MHT, Duangthip D, Wong M, Lo E, Chu CH. Randomized Clinical Trial of 12% and 38% Silver Diamine Fluoride Treatment. J Dent Res. 2018;97(2):171-9. [Google Scholar] [Crossref]
- Llodra JC, Rodriguez A, Ferrer B, Menardia V, Ramos T, Morato M. Efficacy of silver diamine fluoride for caries reduction in primary teeth and first permanent molars of schoolchildren: 36-Month clinical trial. J Dent Res. 2005;84(8):721-5. [Google Scholar] [Crossref]
- Guide S. Chairside guide: Silver diamine fluoride in the management of dental caries lesions. Pediatr Dent. 2018;40(6):492-5. [Google Scholar]
- Jiang M, Wong MC, Chu CH, Dai L, Lo EC. Effects of restoring SDF-treated and untreated dentine caries lesions on parental satisfaction and oral health related quality of life of preschool children. J Dent. 2019;88. [Google Scholar] [Crossref]
- Fröhlich TT, Rocha O, Botton G. Does previous application of silver diammine fluoride influence the bond strength of glass ionomer cement and adhesive systems to dentin? Systematic review and meta-analysis. Int J Paediatr Dent. 2020;30(1):85-95. [Google Scholar] [Crossref]